


《中国康复理论与实践》 ›› 2025, Vol. 31 ›› Issue (6): 666-673.doi: 10.3969/j.issn.1006-9771.2025.06.007
顾逸青1,2, 程舒芃1,2, 李勇强1,2, 毛二莉2, 励建安1,2( )
)
收稿日期:2025-02-26
修回日期:2025-04-23
出版日期:2025-06-25
发布日期:2025-06-16
通讯作者:
励建安,E-mail: 作者简介:顾逸青(1998-),女,汉族,江苏南通市人,硕士研究生,主要研究方向:康复医学(重症康复、神经康复)。
GU Yiqing1,2, CHENG Shupeng1,2, LI Yongqiang1,2, MAO Erli2, LI Jian'an1,2()
Received:2025-02-26
Revised:2025-04-23
Published:2025-06-25
Online:2025-06-16
Contact:
E-mail: 摘要:
目的 系统评价成年气管切开患者直接拔管策略与堵管策略的优劣。
方法 构建PICO,检索PubMed、EMbase、Cochrane Liberary、中国知网、万方数据库和中国生物医学文献数据库中有关气管切开后的成年患者拔管措施的文献,检索时限为建库至2025年2月1日。直接拔管组在通过拔管评估后直接拔管,而不包含≥ 24 h堵管;堵管组拔管前实施≥ 24 h堵管,研究类型为随机对照试验(RCT)、队列研究、病例对照研究。采用纽卡斯尔-渥太华量表(NOS)及Cochrane偏倚风险评估量表评估文献质量。采用GRADE对结局指标进行证据质量评价。提取相关信息进行系统综述。
结果 最终纳入6篇文献,发表时间集中于2003年至2020年,来自西班牙、中国、尼泊尔和以色列4个国家,总样本量745例。非RCT研究的NOS评分为6~8分,RCT的Cochrane偏倚风险评估1篇较低,1篇中等。堵管策略包括完全堵管24~48 h后拔管、逐步缩小管径再堵管后拔管、逐步堵管后拔管;直接拔管策略包括通过拔管评估后直接拔管、内镜检查评估通过后直接拔管。与堵管策略对比,直接拔管策略可显著减少拔管时间,有更低的不良反应发生率,两种策略在拔管成功率、肺部感染发生率上无明显差异。在肺部感染和不良反应发生率上,各项研究间结论不一致。GRADE评价拔管成功率和拔管时间为低质量证据,肺部感染和不良反应发生率为极低质量证据。
结论 成年气管切开患者中,直接拔管策略比堵管策略更优,直接拔管策略能缩短拔管时间,减少不良反应,而两种策略在拔管成功率和肺部感染发生率上无明显差异。
中图分类号:
顾逸青, 程舒芃, 李勇强, 毛二莉, 励建安. 成年气管切开患者拔管的直接策略与堵管策略对比的系统综述[J]. 《中国康复理论与实践》, 2025, 31(6): 666-673.
GU Yiqing, CHENG Shupeng, LI Yongqiang, MAO Erli, LI Jian'an. Capping versus non-capping decannulation strategy in adult tracheostomized patients: a systematic review[J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(6): 666-673.
表1
PICO架构"
| 人群(Population) | 干预(Intervention) | 比较(Comparison) | 结局(Outcome) |
|---|---|---|---|
| 气管切开患者 | 干预场所 | 气管切开患者拔管的直接拔管策略和堵管策略的比较 堵管组(对照) 堵管≥ 24 h后实施拔管 | 拔管成功率 |
| 年龄≥ 18岁 | 医院(重症监护室、康复科病房) | 拔管时间 | |
| 康复服务中心 | 肺部感染 | ||
| 干预人员 | 不良反应 | ||
| 医生 | |||
| 护士 | |||
| 干预措施 | |||
| 对通过拔管评估的患者直接拔管,而不进行≥ 24 h的堵管 |

图1
文献筛选流程图"
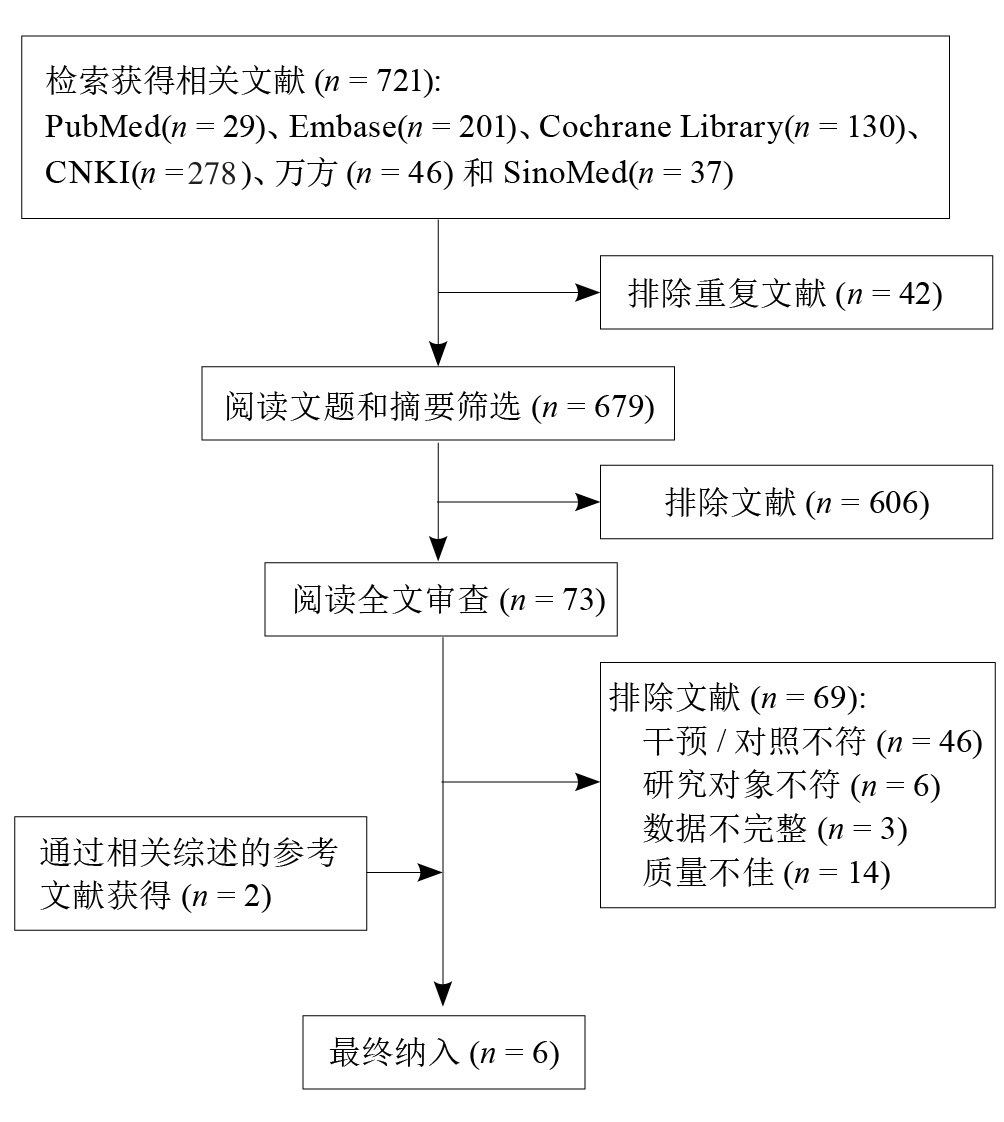
表2
纳入文献质量评价"
| 纳入文献 | NOS评估 | Cochrane偏倚风险评估 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 研究人群选择 | 组间可比性 | 结果测量 | 总分 | 随机序列生成 | 分配隐藏 | 研究者与受试者盲法 | 结果评估盲法 | 数据 不完整 | 选择性报告 | 其他偏倚 | |
| Hernández Martínez等[ | + | + | ? | + | + | + | ? | ||||
| Shrestha等[ | ? | - | - | ? | ? | + | ? | ||||
| Cohen等[ | 3 | 1 | 2 | 6 | |||||||
| 廖圣芳等[ | 4 | 2 | 2 | 8 | |||||||
| 刘玲玲等[ | 3 | 2 | 2 | 7 | |||||||
| 夏嘉川等[ | 4 | 2 | 2 | 8 | |||||||
表3
纳入文献基本信息"
| 纳入文献 | 研究类型 | 国家 | n | 女性比例/% | 年龄/岁 | 直接拔管组 | 堵管组 | 气管套管是否带气囊 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 措施 | n | 措施 | n | |||||||
| Hernández Martínez等[ | RCT | 西班牙 | 330 | 31.8 | 58.3±15.1 | 直接拔管 | 169 | 24 h堵管 | 161 | 是 |
| Shrestha等[ | RCT | 尼泊尔 | 118 | 16.9 | 34.0±13.2 | 直接拔管 | 50 | 24~48 h堵管 | 68 | NA |
| Cohen等[ | 病例对照研究 | 以色列 | 49 | 36.7 | 61.6±17.7 | 内镜检查后直接拔管 | 29 | 缩小管径后堵管 | 20 | 是 |
| 廖圣芳等[ | 病例对照研究 | 中国 | 122 | 27.9 | 38.0 | 直接拔管 | 61 | 24~48 h堵管 | 61 | 是 |
| 刘玲玲等[ | 病例对照研究 | 中国 | 52 | 26.9 | 45.3±15.5 | 直接拔管 | 26 | 24~48 h堵管 | 26 | 否 |
| 夏嘉川等[ | 病例对照研究 | 中国 | 74 | 29.7 | 63.2±11.5 | 直接拔管 | 37 | 部分堵管至全堵管 | 37 | NA |
表4
纳入文献的拔管评估"
| 纳入文献 | 拔管时意识状态 | 生命体征 | 咳嗽能力 | 吞咽能力 | 气道分泌物 | 气道通畅性 |
|---|---|---|---|---|---|---|
| Hernández Martínez等[ | 清醒 | + | + | 部分内镜检查 | 吸痰频率< 2次/8 h | 部分内镜检查 |
| Shrestha等[ | 部分有意识障碍 | + | + | - | + | 部分内镜检查 |
| Cohen等[ | - | + | + | 直接拔管组:内镜检查。堵管组:部分内镜检查 | ||
| 廖圣芳等[ | 部分有意识障碍 | + | + | - | 痰液明显减少> 2 d | - |
| 刘玲玲等[ | 部分有意识障碍 | + | + | - | + | - |
| 夏嘉川等[ | 部分有意识障碍 | + | + | + | - | 部分内镜检查 |
表5
各结局GRADE证据质量"
| 结局指标 | 纳入研究数/n | 研究的局限性 | 不一致性 | 间接性 | 不精确性 | 发表偏倚 | 证据质量 |
|---|---|---|---|---|---|---|---|
| 拔管成功率 | 6[ | 不严重 | 不严重 | 不严重 | 不严重 | 不严重 | 低级 |
| 拔管时间 | 3[ | 不严重 | 不严重 | 不严重 | 不严重 | 不严重 | 低级 |
| 肺部感染 | 3[ | 不严重 | 严重 | 不严重 | 严重 | 不严重 | 极低级 |
| 不良反应 | 3[ | 不严重 | 严重 | 不严重 | 不严重 | 不严重 | 极低级 |
| [1] | PANUGANTI B A, PANG J, FRANCIS D O, et al. Clinicodemographic predictors of tracheotomy tube size and decannulation: a multiinstitutional retrospective cohort study on tracheotomy[J]. Ann Surg, 2023, 277(5): e1138-e1142. |
| [2] | CHOTIRMALL S H, FLYNN M G, DONEGAN C F, et al. Extubation versus tracheostomy in withdrawal of treatment-ethical, clinical, and legal perspectives[J]. J Crit Care, 2010, 25(2): 360.e1-360.e8. |
| [3] | WALLACE S, MCGRATH B A. Laryngeal complications after tracheal intubation and tracheostomy[J]. BJA Educ, 2021, 21(7): 250-257. |
| [4] | SATALOFF R T. Clinical consensus statement: tracheostomy care[J]. Otolaryngol Head Neck Surg, 2013, 149(1): 174. |
| [5] | 中华医学会物理医学与康复学分会心肺康复学组, 中国康复医学会重症康复专业委员会. 成人气管切开拔管中国专家共识(下)[J]. 中华物理医学与康复杂志, 2023, 45(7): 577-584. |
| [6] |
中国残疾人康复协会神经康复专业委员会, 中国康复研究中心, 神经重症气管切开患者气道功能康复与管理专家共识(2024)[J]. 中国康复理论与实践, 2024, 30(8): 869-881.
doi: 10.3969/j.issn.1006-9771.2024.08.001 |
| Committee of Neurological Rehabilitation, China Association of Rehabilitation of Disabled Persons, China Rehabilitation Research Center. Expert consensus on rehabilitation and management of airway function for neurocritical patients with tracheotomy (2024)[J]. Chin J Rehabil Theory Pract, 2024, 30(8): 869-881. | |
| [7] | HERNÁNDEZ G, ORTIZ R, PEDROSA A, et al. La indicación de la traqueotomía condiciona las variables predictoras del tiempo hasta la decanulación en pacientes críticos[J]. Medicina Intensiva, 2012, 36(8): 531-539. |
| [8] | NOWAK A, MARTIN S, HÖHNE M, et al. Tracheal airway pressure in tracheostomy tube capping trials: an experimental study[J]. BMC Pulm Med, 2022, 22(1): 484. |
| [9] | PAGE M J, MCKENZIE J E, BOSSUYT P M, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews[J]. BMJ, 2021, 372: n71. |
| [10] | WELLS G A, TUGWELL P, O'CONNELL D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses[EB/OL]. [2025-02-26]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm. |
| [11] | 曾宪涛, 刘慧, 陈曦, 等. Meta分析系列之四:观察性研究的质量评价工具[J]. 中国循证心血管医学杂志, 2012, 4(4): 297-299. |
| [12] | HIGGINS J P, ALTMAN D G, GØTZSCHE P C, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials[J]. BMJ, 2011, 343: d5928. |
| [13] | 曾宪涛, 包翠萍, 曹世义, 等. Meta分析系列之三:随机对照试验的质量评价工具[J]. 中国循证心血管医学杂志, 2012, 4(3): 183-185. |
| [14] |
GUYATT G, OXMAN A D, AKL E A, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables[J]. J Clin Epidemiol, 2011, 64(4): 383-394.
doi: 10.1016/j.jclinepi.2010.04.026 pmid: 21195583 |
| [15] | HERNÁNDEZ MARTÍNEZ G, RODRIGUEZ M L, VAQUERO M C, et al. High-flow oxygen with capping or suctioning for tracheostomy decannulation[J]. N Engl J Med, 2020, 383(11): 1009-1017. |
| [16] |
SHRESTHA K K, MOHINDRA S, KUMAR SHRESTHA K. How to decannulate tracheostomised severe head trauma patients: a comparison of gradual vs abrupt technique.[J]. Nepal Med Coll J, 2012, 14(3): 207-211.
pmid: 24047017 |
| [17] | COHEN O, TZELNICK S, LAHAV Y, et al. Feasibility of a single-stage tracheostomy decannulation protocol with endoscopy in adult patients[J]. Laryngoscope, 2016, 126(9): 2057-2062. |
| [18] | 廖圣芳, 陈汉民, 张银清, 等. 重型颅脑损伤气管切开术后直接拔管的临床研究[J]. 中国综合临床, 2003, 19(12): 63-64. |
| [19] | 刘玲玲, 尤春景. 脑损伤患者气管切开术后直接拔管的临床研究[J]. 中国康复, 2014, 29(5): 359-361. |
| LIU L L, YOU C J. One-stage decannulation in brain damage patients with tracheotomy[J]. Chin J Rehabil, 2014, 29(5): 359-361. | |
| [20] |
夏嘉川, 罗忠纯, 郭祥奎, 等. 气管切开后拔管策略对拔管成功率的影响[J]. 中国康复理论与实践, 2018, 24(9): 1067-1071.
doi: 10.3969/j.issn.1006-9771.2018.09.016 |
| XIA J C, LUO Z C, GUO X K, et al. Comparison of ways of extubation after tracheotomy[J]. Chin J Rehabil Theory Pract, 2018, 24(9): 1067-1071. | |
| [21] | PANDIAN V, MILLER C R, SCHIAVI A J, et al. Utilization of a standardized tracheostomy capping and decannulation protocol to improve patient safety[J]. Laryngoscope, 2014, 124(8): 1794-1800. |
| [22] | CERIANA P, CARLUCCI A, NAVALESI P, et al. Weaning from tracheotomy in long-term mechanically ventilated patients: feasibility of a decisional flowchart and clinical outcome[J]. Intensive Care Med, 2003, 29(5): 845-848. |
| [23] | STELFOX H T, CRIMI C, BERRA L, et al. Determinants of tracheostomy decannulation: an international survey[J]. Crit Care, 2008, 12(1): R26. |
| [24] |
MUSSA C C, GOMAA D, ROWLEY D D, et al. AARC clinical practice guideline: management of adult patients with tracheostomy in the acute care setting[J]. Respir Care, 2021, 66(1): 156-169.
doi: 10.4187/respcare.08206 pmid: 32962998 |
| [25] | Korean Bronchoesophagological Society Guideline Task Force, NAM I C, SHIN Y S, et al. Guidelines for tracheostomy from the Korean bronchoesophagological society[J]. Clin Exp Otorhinolaryngol, 2020, 13(4): 361-375. |
| [26] | TROUILLET J L, COLLANGE O, BELAFIA F, et al. Tracheotomy in the intensive care unit: guidelines from a French expert panel[J]. Ann Intensive Care, 2018, 8(1): 37. |
| [27] | EPSTEIN S K. Anatomy and physiology of tracheostomy[J]. Respir Care, 2005, 50(4): 476-482. |
| [28] | 胡银, 青晨, 袁梅, 等. 神经外科气管切开患者拔管指征的最佳证据总结[J]. 中华现代护理杂志, 2023, 29(21): 2847-2854. |
| HU Y, QING C, YUAN M, et al. Best evidence summary of indications for extubation in neurosurgical tracheotomy patients[J]. Chin J Mod Nurs, 2023, 29(21): 2847-2854. | |
| [29] | 牛光宇, 连素娜, 刘仲楠, 等. 全国各级医疗机构关于气管切开套管拔管临床实践情况的调查[J]. 中华结核和呼吸杂志, 2022, 45(8): 762-767. |
| NIU G Y, LIAN S N, LIU Z N, et al. A survey on clinical practice of tracheostomy decannulation in medical institutions at all levels across the country[J]. Chin J Tuberc Respir Dis, 2022, 45(8): 762-767. | |
| [30] | 丁玉菊, 徐绍侠, 张伟, 等. 神经重症气管切开患者拔管临床指征的Meta分析[J]. 中华危重病急救医学, 2019, 31(11): 1378-1383. |
| DING Y J, XU S X, ZHANG W, et al. Indication of tracheostomy extubation in patients with severe neuropathy: a meta-analysis[J]. Chin Crit Care Med, 2019, 31(11): 1378-1383. | |
| [31] | 徐锐, 张济源, 覃家德, 等. 气管切开术后245例直接拔管的认识和体会[J]. 中国临床神经外科杂志, 2012, 17(4): 244-245. |
| [32] |
DAWSON D. Essential principles: tracheostomy care in the adult patient[J]. Nurs Crit Care, 2014, 19(2): 63-72.
doi: 10.1111/nicc.12076 pmid: 24529106 |
| [33] | NINAN A, GRUBB L M, BRENNER M J, et al. Effectiveness of interprofessional tracheostomy teams: a systematic review[J]. J Clin Nurs, 2023, 32(19/20): 6967-6986. |
| [34] | KUTSUKUTSA J, KUUPIEL D, MONORI-KISS A, et al. Tracheostomy decannulation methods and procedures for assessing readiness for decannulation in adults: a systematic scoping review[J]. Int J Evid Based Healthc, 2019, 17(2): 74-91. |
| [35] |
SANTUS P, GRAMEGNA A, RADOVANOVIC D, et al. A systematic review on tracheostomy decannulation: a proposal of a quantitative semiquantitative clinical score[J]. BMC Pulm Med, 2014, 14: 201.
doi: 10.1186/1471-2466-14-201 pmid: 25510483 |
| [36] | SANCHEZ-GUERRERO J A, GUERLAIN J, CEBRIÀ I IRANZO M À, et al. Expiratory airflow obstruction due to tracheostomy tube: a spirometric study in 50 patients[J]. Clin Otolaryngol, 2020, 45(5): 703-709. |
| [37] |
CARTER A, FLETCHER S J, TUFFIN R. The effect of inner tube placement on resistance and work of breathing through tracheostomy tubes: a bench test[J]. Anaesthesia, 2013, 68(3): 276-282.
doi: 10.1111/anae.12094 pmid: 23278349 |
| [38] |
WARNECKE T, SUNTRUP S, TEISMANN I K, et al. Standardized endoscopic swallowing evaluation for tracheostomy decannulation in critically ill neurologic patients[J]. Crit Care Med, 2013, 41(7): 1728-1732.
doi: 10.1097/CCM.0b013e31828a4626 pmid: 23774336 |
| [39] |
MORRIS L L. Capping a cuffed tracheostomy tube[J]. Crit Care Nurse, 2012, 32(2): 12-13.
doi: 10.4037/ccn2012391 |
| [40] |
VILLALBA D, FELD V, LEIVA V, et al. Effect of tracheostomy tube on work of breathing: comparison of pre- and post-decannulation[J]. Int J Crit Illn Inj Sci, 2016, 6(3): 98-102.
pmid: 27722109 |
| [41] | SHI Z H, JONKMAN A, DE VRIES H, et al. Expiratory muscle dysfunction in critically ill patients: towards improved understanding[J]. Intensive Care Med, 2019, 45(8): 1061-1071. |
| [42] | ZANATA IDE L, SANTOS R S, HIRATA G C. Tracheal decannulation protocol in patients affected by traumatic brain injury[J]. Int Arch Otorhinolaryngol, 2014, 18(2): 108-114. |
| [43] |
GALLICE T, CUGY E, BRANCHARD O, et al. Predictive factors for successful decannulation in patients with tracheostomies and brain injuries: a systematic review[J]. Dysphagia, 2024, 39(4): 552-572.
doi: 10.1007/s00455-023-10646-2 pmid: 38189928 |
| [44] |
DZIEWAS R, STELLATO R, VAN DER TWEEL I, et al. Pharyngeal electrical stimulation for early decannulation in tracheotomised patients with neurogenic dysphagia after stroke (PHAST-TRAC): a prospective, single-blinded, randomised trial[J]. Lancet Neurol, 2018, 17(10): 849-859.
doi: S1474-4422(18)30255-2 pmid: 30170898 |
| [45] | LANINI B, BINAZZI B, ROMAGNOLI I, et al. Tracheostomy decannulation in severe acquired brain injury patients: the role of flexible bronchoscopy[J]. Pulmonology, 2023, 29(Suppl 4): S80-S85. |
| [46] | MARTIN K A, COLE T D K, PERCHA C M, et al. Standard versus accelerated speaking valve placement after percutaneous tracheostomy: a randomized controlled feasibility study[J]. Ann Am Thorac Soc, 2021, 18(10): 1693-1701. |
| [1] | 王梅, 朱文平. 身体活动干预2型糖尿病患者的健康效益:系统综述的系统综述[J]. 《中国康复理论与实践》, 2025, 31(5): 553-560. |
| [2] | 叶绿, 常晶, 凌海润. 网络行为成瘾的运动干预效果:系统综述的系统综述[J]. 《中国康复理论与实践》, 2025, 31(4): 431-440. |
| [3] | 朱志强, 徐巧玲, 邵雪云. 肥胖和超重儿童参与身体活动的健康效益:系统综述的系统综述[J]. 《中国康复理论与实践》, 2025, 31(3): 296-305. |
| [4] | 蔡倩, 张溪, 苏海荣, 刘娜, 黄颖, 李际强, 夏金根, 郑德采. 吸气肌训练对脱机失败者脱机疗效的系统综述[J]. 《中国康复理论与实践》, 2025, 31(3): 306-313. |
| [5] | 徐晓红, 钟晓珂, 孙思怡, 张祁, 程怀春. 轻度认知障碍老年人参与艺术治疗心理健康效益的系统综述[J]. 《中国康复理论与实践》, 2025, 31(2): 165-171. |
| [6] | 杨文睿, 崔思栋, 曾莉. 虚拟与增强现实对孤独症谱系障碍儿童青少年认知、情绪和适应性行为干预效果的系统综述[J]. 《中国康复理论与实践》, 2024, 30(9): 1026-1033. |
| [7] | 周静, 张晓晓, 丁忠冰, 陈建超, 魏星星, 林姝琦. 智力与发展性残疾儿童言语与语言障碍康复的系统综述[J]. 《中国康复理论与实践》, 2024, 30(8): 894-902. |
| [8] | 杨家坤, 张晓侠. 适应性体育活动对智力与发展性残疾儿童功能、活动和参与效益的系统综述[J]. 《中国康复理论与实践》, 2024, 30(7): 768-777. |
| [9] | 唐乐天, 黄兆欣, 刘超, 肖晓飞. 前交叉韧带重建术后患者高血流限制训练康复效果的系统综述[J]. 《中国康复理论与实践》, 2024, 30(7): 789-796. |
| [10] | 魏晓微. 数字赋能技术促进智力与发展性残疾儿童身体活动和健康的系统综述[J]. 《中国康复理论与实践》, 2024, 30(5): 497-504. |
| [11] | 王红志, 杨剑. 虚拟现实技术在脑性瘫痪儿童青少年身体活动和健康中的应用:系统综述的系统综述[J]. 《中国康复理论与实践》, 2024, 30(5): 505-512. |
| [12] | 钟晓珂, 王琦, 昌思琴, 蒋长好. 长期身体活动对孤独症谱系障碍儿童执行功能效果的系统综述[J]. 《中国康复理论与实践》, 2024, 30(5): 535-542. |
| [13] | 吴佳洺, 张青, 武爱红. 智力与发展性残疾儿童青少年音乐干预的功能、健康和发展效益:系统综述的系统综述[J]. 《中国康复理论与实践》, 2024, 30(5): 543-553. |
| [14] | 喜悦, 杨剑. 不同身体活动对脑性瘫痪儿童青少年健康效益的系统综述[J]. 《中国康复理论与实践》, 2024, 30(2): 157-167. |
| [15] | 张皓媛, 田罡, 李雪峰, 李鸿江, 闵红巍, 唐鹏, 张睿, 顾蕊, 刘克敏. 糖尿病足截肢者临床及康复特征对其预后影响的系统综述[J]. 《中国康复理论与实践》, 2024, 30(11): 1281-1290. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
|
||