


《中国康复理论与实践》 ›› 2021, Vol. 27 ›› Issue (7): 819-828.doi: 10.3969/j.issn.1006-9771.2021.07.014
郑志昌1,袁玮2,林伟1,刘杰1,王晓荣1,杨威1,于海涛1,薛淞1,王亚敏1,唐丽1,王国栋1( )
)
收稿日期:2020-07-03
修回日期:2020-10-26
出版日期:2021-07-25
发布日期:2021-07-28
通讯作者:
王国栋
E-mail:lukewang1972@sohu.com
作者简介:郑志昌(1980-),男,汉族,河南洛阳市人,硕士,主治医师,主要研究方向:冠心病、心脏康复。|王国栋(1972-),男,汉族,山东诸城市人,博士,副主任医师,主要研究方向:冠心病、心脏康复。
基金资助:
ZHENG Zhi-chang1,YUAN Wei2,LIN Wei1,LIU Jie1,WANG Xiao-rong1,YANG Wei1,YU Hai-tao1,XUE Song1,WANG Ya-min1,TANG Li1,WANG Guo-dong1()
Received:2020-07-03
Revised:2020-10-26
Published:2021-07-25
Online:2021-07-28
Contact:
WANG Guo-dong
E-mail:lukewang1972@sohu.com
Supported by:摘要:
目的 通过基于心肺运动试验(CPET)的测试数据和患者的一般临床资料,对稳定型冠心病患者进行心脏康复风险分层,区分出心脏康复的低危和高危患者。
方法 连续纳入2014年12月至2018年12月本院冠心病数据库中冠脉造影术前行CPET检查的稳定型冠心病患者114例。使用LASSO回归进行变量筛选;使用Logistic回归建立评估模型,使用R软件的RMS包绘制评估模型的列线图;通过R软件的ROCR包绘制受试者工作特征曲线,计算曲线下面积(AUC)。
结果 根据LASSO回归分析,确定7个预测因素:冠脉造影结果、最大二氧化碳通气当量(EqCO2max)、淋巴细胞计数、空腹血糖水平、心肌酶阳性、血同型半胱氨酸和血尿素氮水平。结合临床经验及权重分析,最终纳入冠脉造影结果、EqCO2max、淋巴细胞计数和空腹血糖水平4个因素进行Logistic回归建模;模型的AUC值为0.875,对结局事件有良好预测能力。
结论 EqCO2max和淋巴细胞计数为稳定型冠心病患者心脏康复风险分层的主要预测因素,可用于识别稳定型冠心病心脏康复的高危患者;基于CPET和实验室检查建立的稳定型冠心病患者心脏康复风险分层评估模型,可以为稳定型冠心病患者心脏康复的风险评估提供帮助。
中图分类号:
郑志昌,袁玮,林伟,刘杰,王晓荣,杨威,于海涛,薛淞,王亚敏,唐丽,王国栋. 稳定型冠心病患者心脏康复的风险分层模型[J]. 《中国康复理论与实践》, 2021, 27(7): 819-828.
ZHENG Zhi-chang,YUAN Wei,LIN Wei,LIU Jie,WANG Xiao-rong,YANG Wei,YU Hai-tao,XUE Song,WANG Ya-min,TANG Li,WANG Guo-dong. A Risk Prediction Model for Cardiac Rehabilitation in Patients with Stable Coronary Artery Disease[J]. 《Chinese Journal of Rehabilitation Theory and Practice》, 2021, 27(7): 819-828.
表1
两组一般资料比较(n = 114) "
| 项目 | 风险分层 | t/χ2值 | P值 | |
|---|---|---|---|---|
| 低危组(n = 100) | 高危组(n = 14) | |||
| 年龄(岁) | 59.490±7.543 | 60.210±8.210 | -0.333 | 0.740 |
| 性别(n) | 5.363 | 0.021 | ||
| 男 | 53 | 12 | ||
| 女 | 47 | 2 | ||
| 体质量指数(kg/m2) | 26.288±3.384 | 25.179±1.882 | 1.197 | 0.234 |
| 高血压病史(n) | 65 | 12 | 2.404 | 0.121 |
| 糖尿病史(n) | 35 | 4 | 0.225 | 0.635 |
| 高血脂病史(n) | 66 | 11 | 0.885 | 0.347 |
| 卒中病史(n) | 4 | 1 | 0.289 | 0.591 |
| 吸烟(n) | 6.805 | 0.078 | ||
| 不吸烟 | 58 | 5 | ||
| 吸烟、已戒 | 17 | 1 | ||
| 吸烟、未戒 | 25 | 8 | ||
| 饮酒(n) | 6.325 | 0.097 | ||
| 不饮酒 | 64 | 6 | ||
| 饮酒、已戒 | 10 | 0 | ||
| 饮酒、未戒 | 26 | 8 | ||
表2
两组实验室检查比较(n = 114) "
| 实验室检查 | 风险分层 | t/Z/χ2值 | P值 | |
|---|---|---|---|---|
| 低危组(n = 100) | 高危组(n = 14) | |||
| 白细胞(×109 /L) | 6.410±1.615 | 7.00(4.750, 8.000) | -0.457 | 0.648 |
| 中性粒细胞(×109 /L) | 4.155±1.398 | 4.941±3.075 | -1.639 | 0.104 |
| 淋巴细胞(×109 /L) | 1.811±0.607 | 1.496±0.409 | 1.871 | 0.020 |
| 红细胞(×1012 /L) | 4.770±1.214 | 4.50(4.000, 5.000) | -0.852 | 0.394 |
| 血小板(×109 /L) | 223.390±50.789 | 215.710±58.950 | 0.519 | 0.605 |
| 总胆固醇(mmol/L) | 4.130±0.895 | 4.290±1.267 | -0.577 | 0.565 |
| 甘油三酯(mmol/L) | 1.630±1.253 | 1.400(1.000, 2.000) | -0.216 | 0.829 |
| 低密度脂蛋白胆固醇(mmol/L) | 2.460±0.731 | 2.570±0.852 | -0.524 | 0.602 |
| 高密度脂蛋白胆固醇(mmol/L) | 1.120±0.409 | 1.000(0.900, 1.100) | -0.346 | 0.729 |
| 空腹血糖(mmol/L) | 5.970±1.766 | 7.210±3.401 | -2.153 | 0.033 |
| 超敏C反应蛋白 (mg/dL) | 0.530±0.429 | 0.200(0.100, 0.625) | -0.757 | 0.449 |
| 同型半胱氨酸 (μmol/L) | 12.480±4.631 | 16.710±12.003 | -2.484 | 0.014 |
| 尿素氮(mmol/L) | 5.320±1.377 | 5.860±1.956 | -1.293 | 0.199 |
| 肌酐(μmol/L) | 68.410±16.261 | 72.790±28.110 | -0.850 | 0.397 |
| 尿酸(μmol/L) | 331.540±100.749 | 345.140±119.413 | -0.462 | 0.645 |
| CK-MB阳性(n) | 0 | 3 | 15.001 | 0.006 |
| 造影结果(n) | 7.602 | 0.006 | ||
| 阴性 | 37 | 0 | ||
| 阳性 | 63 | 14 | ||
表3
两组CPET参数比较(n = 114) "
| CPET | 风险分层 | t/Z值 | P值 | |
|---|---|---|---|---|
| 低危组(n = 100) | 高危组(n = 14) | |||
| Loadmax (W) | 99.910±31.455 | 102.930±24.550 | -0.344 | 0.731 |
| VEmax (L/min) | 47.910±13.419 | 52.070±11.552 | -1.103 | 0.272 |
| AT (ml/min) | 879.430±215.891 | 937.860±238.943 | -0.936 | 0.351 |
| VO2max (ml/min) | 1341.000±343.888 | 1339.430±259.536 | 0.016 | 0.987 |
| HRmax (次/min) | 160±8 | 159±8 | 0.890 | 0.375 |
| VO2/HR (ml/次) | 10.959±2.362 | 11.471±2.176 | -0.765 | 0.446 |
| VCO2max (ml/min) | 1508.780±451.536 | 1532.50±371.499 | -0.188 | 0.851 |
| EqCO2max | 30.689±3.803 | 33.343±4.770 | -2.368 | 0.020 |
| EqCO2-AT | 31.050±4.498 | 32.570±4.327 | -1.191 | 0.236 |
| RER | 1.117±0.090 | 1.150(1.107, 1.203) | -1.270 | 0.204 |
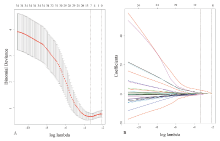
图1
预测因素筛选 注: A.进行交叉验证,选择最优的惩罚系数lambda,在最优lambda时,筛选出7个候选因素;B.选择交叉验证误差最小的lambda,其数值为0.03568472"


图2
纳入7个预测因素的模型"
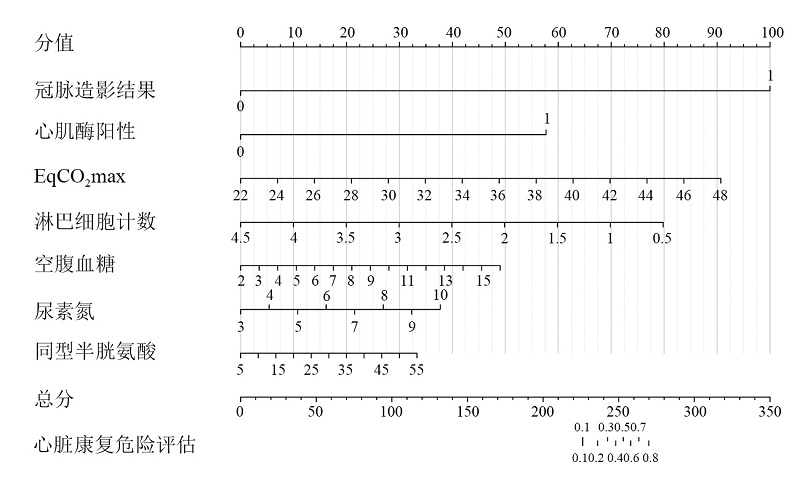

图3
纳入6个预测因素的模型"
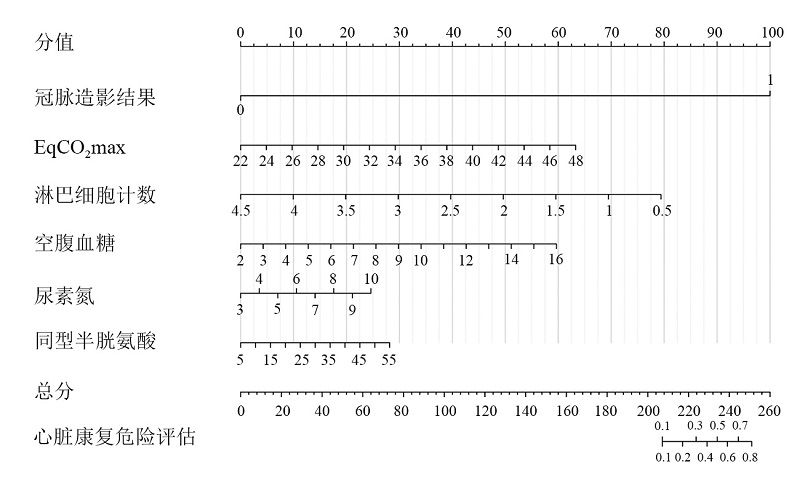

图4
纳入4个预测因素的模型"
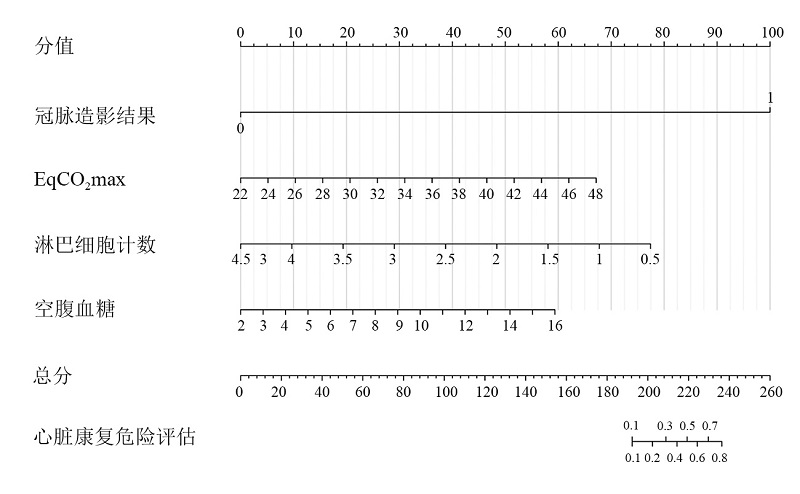

图5
ROC曲线图"
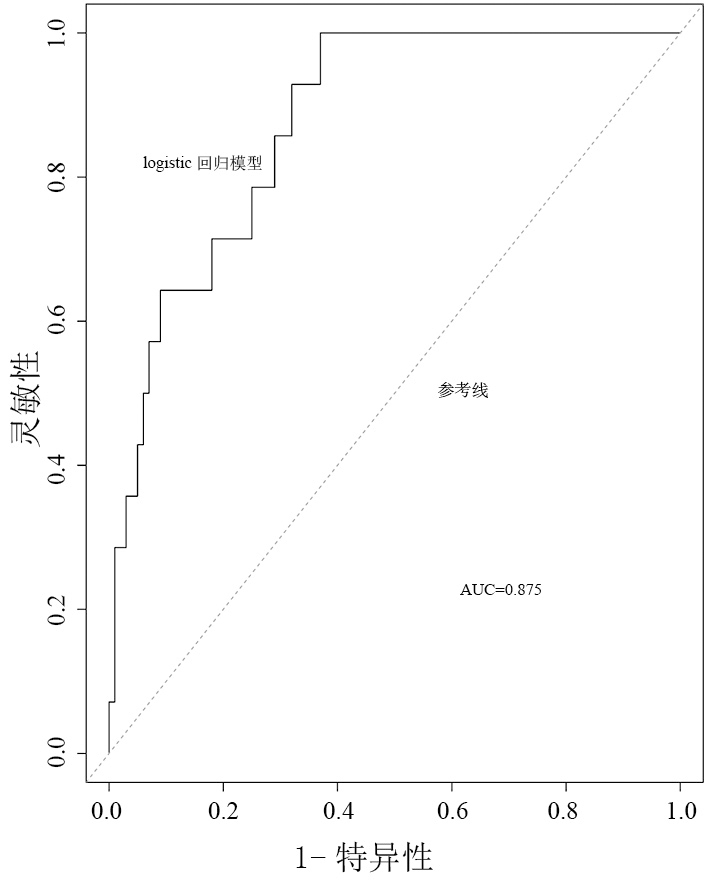
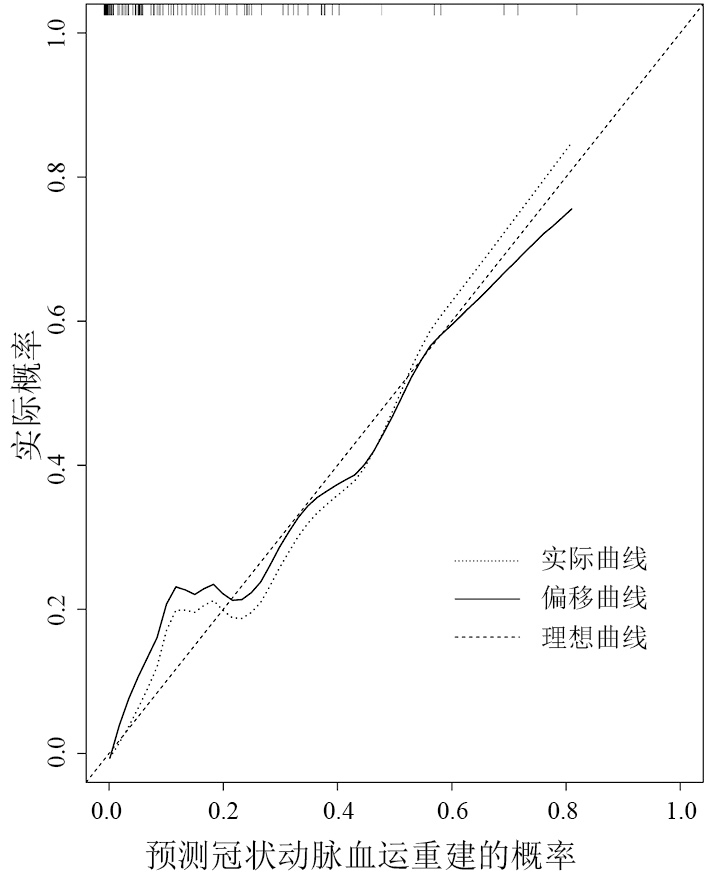
图6
校准曲线"
| [1] | ANDERSON L, OLDRIDGE N, THOMPSON D R, et al. Exercise-based cardiac rehabilitation for coronary heart disease: cochrane systematic review and meta-analysis[J]. J Am Coll Cardiol, 2016, 67(1):1-12. |
| [2] | THOMAS R J, BALADY G, BANKA G, et al. 2018 ACC/AHA Clinical Performance and Quality Measures for Cardiac Rehabilitation: a report of the American College of Cardiology/American Heart Association Task Force on performance measures[J]. Circ Cardiovasc Qual Outcomes, 2018, 11(4):e000037. |
| [3] |
Writing Committee Members, THOMAS R J, KING M, et al. AACVPR/ACCF/AHA 2010 update: performance measures on cardiac rehabilitation for referral to cardiac rehabilitation/secondary prevention services: a report of the American Association of Cardiovascular and Pulmonary Rehabilitation and the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Clinical Performance Measures for Cardiac Rehabilitation)[J]. Circulation, 2010, 122(13):1342-1350.
doi: 10.1161/CIR.0b013e3181f5185b |
| [4] |
SMITH S C, BENJAMIN E J, BONOW R O, et al. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and Other Atherosclerotic Vascular Disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation[J]. Circulation, 2011, 124(22):2458-2473.
doi: 10.1161/CIR.0b013e318235eb4d |
| [5] | 中国康复医学会心血管病专业委员会. 中国心脏康复与二级预防指南2018精要[J]. 中华内科杂志, 2018, 57(11):802-810. |
| Cardiovascular Disease Committee of the Chinese Society of Rehabilitation Medicine. Highlights of Guidelines for Cardiac Rehabilitation and Secondary Prevention in China 2018[J]. Chin J Internal Med, 2018, 57(11):802-810. | |
| [6] |
SANTOS A A, SILVA A K, VANDERLEI F M, et al. Analysis of agreement between cardiac risk stratification protocols applied to participants of a center for cardiac rehabilitation[J]. Braz J Phys Ther, 2016, 20(4):298-305.
doi: 10.1590/bjpt-rbf.2014.0159 |
| [7] | SILVA A K, BARBOSA M P, BERNARDO A F, et al. Cardiac risk stratification in cardiac rehabilitation programs: a review of protocols[J]. Rev Bras Cir Cardiovasc, 2014, 29(2):255-265. |
| [8] |
KNUUTI J, WIJNS W, SARASTE A, et al. 2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes[J]. Eur Heart J, 2020, 41(3):407-477.
doi: 10.1093/eurheartj/ehz425 |
| [9] |
YANG E, TAYLOR A. Comparing American and European Guidelines for the initial diagnosis of stable ischaemic heart disease[J]. Eur Heart J, 2020, 41(7):811-815.
doi: 10.1093/eurheartj/ehaa057 |
| [10] |
SANTORO C, SORRENTINO R, ESPOSITO R, et al. Cardiopulmonary exercise testing and echocardiographic exam: an useful interaction[J]. Cardiovasc Ultrasound, 2019, 17(1):29.
doi: 10.1186/s12947-019-0180-0 |
| [11] | GUAZZI M, ARENA R, HALLE M, et al. 2016 Focused update: clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations[J]. Circulation, 2016, 133(24):e694-e711. |
| [12] |
American Thoracic Society, American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing[J]. Am J Respir Crit Care Med, 2003, 167(2):211-277.
doi: 10.1164/rccm.167.2.211 |
| [13] | SIETSEMA K E, STRINGER W W, SUE D Y, et al. Wasserman & Whipp's: Principles of Exercise Testing and Interpretation: Including Pathophysiology and Clinical Applications[M]. Lippincott Williams & Wilkins, 2020. |
| [14] | 中华医学会心血管病学分会介入心脏病学组, 中国医师协会心血管内科医师分会血栓防治专业委员会, 中华心血管病杂志编辑委员会. 中国经皮冠状动脉介入治疗指南(2016)[J]. 中华心血管病杂志, 2016, 44(5):382-400. |
| Interventional Cardiology Group of the Chinese Society of Cardiovascular Medicine, Thrombosis Prevention and Control Committee of Cardiovascular Physicians Branch of China Medical Association, Editorial Board of Chinese Journal of Cardiology. Guidelines for Percutaneous Coronary Intervention in China ( 2016 )[J]. Chin J Cardiol 2016, 44(5):382-400. | |
| [15] |
NEUMANN F J, SOUSA-UVA M, AHLSSON A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization[J]. Eur Heart J, 2019, 40(2):87-165.
doi: 10.1093/eurheartj/ehy394 |
| [16] |
STEYERBERG E W, VERGOUWE Y. Towards better clinical prediction models: seven steps for development and an ABCD for validation[J]. Eur Heart J, 2014, 35(29):1925-1931.
doi: 10.1093/eurheartj/ehu207 |
| [17] |
DUNLAY S M, WITT B J, ALLISON T G, et al. Barriers to participation in cardiac rehabilitation[J]. Am Heart J, 2009, 158(5):852-859.
doi: 10.1016/j.ahj.2009.08.010 |
| [18] |
TIAN Y, DENG P, LI B, et al. Treatment models of cardiac rehabilitation in patients with coronary heart disease and related factors affecting patient compliance[J]. Rev Cardiovasc Med, 2019, 20(1):27-33.
doi: 10.31083/j.rcm.2019.01.53 |
| [19] |
ROFFI M, PATRONO C, COLLET J P, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2016, 37(3):267-315.
doi: 10.1093/eurheartj/ehv320 |
| [20] |
GUAZZI M, BANDERA F, OZEMEK C, et al. Cardiopulmonary exercise testing: what is its value?[J]. J Am Coll Cardiol, 2017, 70(13):1618-1636.
doi: 10.1016/j.jacc.2017.08.012 |
| [21] | HERDY A H, RITT L E, STEIN R, et al. Cardiopulmonary exercise test: background, applicability and interpretation[J]. Arq Bras Cardiol, 2016, 107(5):467-481. |
| [22] |
AKINCI OZYUREK B, SAVAS BOZBAS S, AYDINALP A, et al. Value of cardiopulmonary exercise testing in the diagnosis of coronary artery disease[J]. Tuberk Toraks, 2019, 67(2):102-107.
doi: 10.5578/tt.68200 |
| [23] |
POPOVIC D, MARTIC D, DJORDJEVIC T, et al. Oxygen consumption and carbon-dioxide recovery kinetics in the prediction of coronary artery disease severity and outcome[J]. Int J Cardiol, 2017, 248:39-45.
doi: 10.1016/j.ijcard.2017.06.107 |
| [24] |
SHAMLOO A S, DINOV B, BERTAGNOLLI L, et al. Value of cardiogoniometry in diagnosis of coronary artery disease in patients with suspected stable ischemic heart disease: a systematic review and meta-analysis[J]. Int Heart J, 2019, 60(3):527-538.
doi: 10.1536/ihj.18-391 |
| [25] |
MAZAHERI R, SHAKERIAN F, VASHEGHANI-FARAHANI A, et al. The usefulness of cardiopulmonary exercise testing in assessment of patients with suspected coronary artery disease[J]. Postgrad Med J, 2016, 92(1088):328-332.
doi: 10.1136/postgradmedj-2015-133576 |
| [26] |
DEVUYST S, GIGASE A, SPAPEN J, et al. Impact of non-invasive anatomical testing on optimal medical prescription in patients with suspected coronary artery disease[J]. Cardiovasc Diagn Ther, 2019, 9(3):221-228.
doi: 10.21037/cdt |
| [27] |
SCHIEFER R, RICKLI H, NEURAUTER E, et al. Non-invasive assessment prior to invasive coronary angiography in routine clinical practice in Switzerland: is it according to the guidelines?[J]. PLoS One, 2019, 14(9):e0222137.
doi: 10.1371/journal.pone.0222137 |
| [28] |
HEINZE G, WALLISCH C, DUNKLER D. Variable selection: a review and recommendations for the practicing statistician[J]. Biom J, 2018, 60(3):431-449.
doi: 10.1002/bimj.v60.3 |
| [29] |
MOONS K G, KENGNE A P, WOODWARD M, et al. Risk prediction models: I. Development, internal validation, and assessing the incremental value of a new (bio)marker[J]. Heart, 2012, 98(9):683-690.
doi: 10.1136/heartjnl-2011-301246 |
| [30] |
SCIORATI C, RIGAMONTI E, MANFREDI A A, et al. Cell death, clearance and immunity in the skeletal muscle[J]. Cell Death Differ, 2016, 23(6):927-937.
doi: 10.1038/cdd.2015.171 |
| [31] |
STAKOS D A, KAMBAS K, KONSTANTINIDIS T, et al. Expression of functional tissue factor by neutrophil extracellular traps in culprit artery of acute myocardial infarction[J]. Eur Heart J, 2015, 36(22):1405-1414.
doi: 10.1093/eurheartj/ehv007 |
| [32] |
KINGMA J G. Effect of platelet GPIIb/IIIa receptor blockade with MK383 on infarct size and myocardial blood flow in a canine reocclusion model[J]. J Cardiovasc Pharmacol Ther, 2019, 24(2):182-192.
doi: 10.1177/1074248418808389 |
| [33] |
ALTINTAS O, ALTINTAS M O, TASAL A, et al. The relationship of platelet-to-lymphocyte ratio with clinical outcome and final infarct core in acute ischemic stroke patients who have undergone endovascular therapy[J]. Neurol Res, 2016, 38(9):759-765.
doi: 10.1080/01616412.2016.1215030 |
| [34] |
YU Y, ZHOU Z, SUN K, et al. Association between coronary artery atherosclerosis and plasma glucose levels assessed by dual-source computed tomography[J]. J Thorac Dis, 2018, 10(11):6050-6059.
doi: 10.21037/jtd |
| [35] | HUANG Y, CAI X, MAI W, et al. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis[J]. BMJ, 2016, 355:i5953. |
| [1] | 曹雨菡, 李瑾, 何民, 王丹, 陈伟. 基于ICF冠心病患者远程康复的Scoping综述[J]. 《中国康复理论与实践》, 2023, 29(4): 433-442. |
| [2] | 李慕瑶, 王梅, 杜亮, 童露, 许三雄. 基于WHO-FICs架构有氧联合抗阻运动对老年冠心病并发高血压患者的效果[J]. 《中国康复理论与实践》, 2023, 29(3): 326-334. |
| [3] | 秦宁,沈志莹,石双姣,李旭红,钟竹青. 心脏康复转介服务[J]. 《中国康复理论与实践》, 2022, 28(3): 366-372. |
| [4] | 蔡玮,邢文华,梁文平,赵雷,刘萍,滕珲,王国栋. 南皮县经皮冠状动脉介入治疗术后患者心脏康复现状调查[J]. 《中国康复理论与实践》, 2021, 27(8): 966-972. |
| [5] | 曾斌,刘亚康,王龙平,张鸣生. 慢性阻塞性肺疾病患者通气有效性与运动后心脏功能的关系[J]. 《中国康复理论与实践》, 2021, 27(7): 812-818. |
| [6] | 袁玮,聂姗,贾楠,郑志昌,王浩彦. 运动康复对经皮冠状动脉介入术后急性冠状动脉综合征患者的效果[J]. 《中国康复理论与实践》, 2021, 27(2): 208-215. |
| [7] | 于曼丽,姜衡,李彬,柴丽莉,沈慧,施峰,谢东峰,林兴中. 太极拳对老年心肌梗死后心力衰竭患者心脏功能的效果[J]. 《中国康复理论与实践》, 2020, 26(8): 969-974. |
| [8] | 司旭艳, 王世广, 王鹏. 生理性缺血训练在心脏康复中的研究进展[J]. 《中国康复理论与实践》, 2020, 26(6): 683-686. |
| [9] | 张穗浩, 林峰, 董少红. 高强度间歇训练在急性心肌梗死介入治疗术后的应用现状[J]. 《中国康复理论与实践》, 2019, 25(6): 696-699. |
| [10] | 刘功亮, 杨坚, 王人卫, 李擎, 范利. 冠心病康复有氧运动不同强度设定方法的一致性研究[J]. 《中国康复理论与实践》, 2018, 24(8): 950-955. |
| [11] | 毛贵如, 王丽姿, 许桢桢, 陈燕娜. 多次住院冠心病患者疾病感知水平的调查分析[J]. 《中国康复理论与实践》, 2017, 23(2): 221-225. |
| [12] | 蔡泽坤综述,徐琳,邱健审校. 远程心电监测在心肌梗死患者心脏康复中的应用进展①[J]. 《中国康复理论与实践》, 2016, 22(1): 75-78. |
| [13] | 孙佩伟;马建新 . 冠心病的康复进展[J]. 《中国康复理论与实践》, 2015, 21(12): 1425-1429. |
| [14] | 周霄云. 中医临床护理路径应用于冠心病患者的效果[J]. 《中国康复理论与实践》, 2013, 19(2): 193-195. |
| [15] | 马跃文;刘畅. 心脏康复对于冠心病患者抑郁、焦虑情绪改善的研究进展[J]. 《中国康复理论与实践》, 2012, 18(2): 141-143. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
|
||