


《中国康复理论与实践》 ›› 2023, Vol. 29 ›› Issue (11): 1346-1352.doi: 10.3969/j.issn.1006-9771.2023.11.013
朱烈烈, 夏建宁, 蒲新宇, 邵湘芝, 张嘉诚, 吴登宠( )
)
收稿日期:2023-08-11
修回日期:2023-10-16
出版日期:2023-11-25
发布日期:2023-11-30
通讯作者:
吴登宠(1983-),男,硕士,副主任医师,主要研究方向:神经康复。E-mail: dcwuwzs@126.com
作者简介:朱烈烈(1978-),男,汉族,浙江温州市人,硕士,副主任医师,主要研究方向:肌骨代谢、营养与康复。
基金资助:
ZHU Lielie, XIA Jianning, PU Xinyu, SHAO Xiangzhi, ZHANG Jiacheng, WU Dengchong()
Received:2023-08-11
Revised:2023-10-16
Published:2023-11-25
Online:2023-11-30
Contact:
WU Dengchong, E-mail: dcwuwzs@126.com
Supported by:摘要:
目的 评价入院时老年营养风险指数(GNRI)预测脑卒中患者康复期(卒中后3个月)神经功能的效能。
方法 2022年11月至2023年1月,温州市中医院住院缺血性脑卒中患者277例,根据卒中后3个月改良Rankin量表(mRS)评分分为预后良好组(n = 195)和预后不良组(n = 82),比较两组临床资料和GNRI。
结果 与预后良好组相比,预后不良组GNRI显著降低(t = -9.569, P < 0.001),高营养风险患者比例显著增多(χ2 = 68.861, P < 0.001);预后不良病例营养风险更高(Z = 65.406, P < 0.001)。校正协变量后,高GNRI水平是卒中后3个月神经功能预后不良发生的独立保护因素(OR = 0.895, 95%CI 0.864~0.927, P < 0.05),且发生神经功能不良预后的风险随着GNRI营养风险等级的增加而逐渐增大。GNRI、国立卫生研究院卒中量表(NIHSS)评分和体质量指数(BMI)的曲线下面积(AUC)分别为0.812 (Z = 11.576, P < 0.001)、0.759 (Z = 8.328, P < 0.001)和0.594 (Z = 2.716, P = 0.007),GNRI和NIHSS联合效能更高(AUC = 0.875, Z = 17.389, P < 0.001)。GNRI、NIHSS评分以及两者联合预测神经功能的敏感性分别为65.85%、76.83%和79.21%,特异性分别为81.54%、60.51%和82.95%。
结论 入院时GNRI与卒中后3个月的神经功能密切相关。GNRI可以单独或联合NIHSS评分用来预测康复期的神经功能,是传统预测指标的有益补充。
中图分类号:
朱烈烈, 夏建宁, 蒲新宇, 邵湘芝, 张嘉诚, 吴登宠. 老年营养风险指数对脑卒中后神经功能预后的效能[J]. 《中国康复理论与实践》, 2023, 29(11): 1346-1352.
ZHU Lielie, XIA Jianning, PU Xinyu, SHAO Xiangzhi, ZHANG Jiacheng, WU Dengchong. Predictive efficacy of Geriatric Nutritional Risk Index on neurological outcome after stroke[J]. 《Chinese Journal of Rehabilitation Theory and Practice》, 2023, 29(11): 1346-1352.
表1
两组一般资料比较(n = 277)"
| 项目 | 预后良好组(n = 195) | 预后不良组(n = 82) | t/χ2/Z值 | P值 |
|---|---|---|---|---|
| 年龄/岁 | 68.5(62.4,74.1) | 72.4(62.6,77.9) | -1.600 | 0.110 |
| 性别(男/女)/n | 117/78 | 27/55 | 16.951 | < 0.001 |
| 家庭年收入超过5万元/n | 161 | 61 | 2.424 | 0.120 |
| 婚姻状态(离异或寡居)/n | 55 | 30 | 1.906 | 0.167 |
| BMI/(kg·m-2) | 24.45±4.16 | 23.01±2.36 | -3.649 | < 0.001 |
| 既往吸烟/n | 63 | 21 | 1.226 | 0.268 |
| 既往饮酒/n | 68 | 36 | 2.008 | 0.157 |
| 并发症/n | ||||
| 高血压病 | 147 | 69 | 2.581 | 0.108 |
| 糖尿病 | 141 | 64 | 0.989 | 0.320 |
| 高脂血症 | 130 | 57 | 0.213 | 0.644 |
| 其他 | 41 | 20 | 0.381 | 0.537 |
| 梗死类型/n | ||||
| TACI | 46 | 13 | 2.444 | 0.295 |
| PACI | 82 | 41 | ||
| POCI | 67 | 28 | ||
| 接受溶栓治疗/n(%) | 89 | 29 | 2.492 | 0.114 |
| NIHSS评分 | 11.01±2.09 | 13.56±2.69 | 7.680 | < 0.001 |
| GNRI | 101.54±10.79 | 88.39±9.54 | -9.569 | < 0.001 |
| GNRI分级/n | ||||
| Q1 | 8 | 30 | 68.861 | < 0.001 |
| Q2 | 27 | 21 | ||
| Q3 | 44 | 15 | ||
| Q4 | 116 | 16 | ||
| mRS评分 | 2(1, 2) | 4(3, 5) | -13.749 | < 0.001 |
表2
GNRI、NIHSS和BMI对神经功能预后不良发生风险的Logistic回归分析"
| 指标 | 模型1 | 模型2 | 模型3 | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95%CI) | P值 | OR (95%CI) | P值 | OR (95%CI) | P值 | |||
| GNRI | 0.889(0.862~0.918) | < 0.001 | 0.889(0.860~0.918) | < 0.001 | 0.895(0.864~0.927)a | < 0.001 | ||
| NIHSS | 1.590(1.387~1.823) | < 0.001 | 1.571(1.366~1.808) | < 0.001 | 1.554(1.318~1.832)b | < 0.001 | ||
| BMI | 0.887(0.816~0.963) | 0.004 | 0.894(0.820~0.974) | 0.010 | 0.899(0.799~1.011)c | 0.077 | ||
表3
GNRI等级对神经功能预后不良发生风险的Logistic回归分析"
| GNRI等级 | n | 模型1 | 模型2 | ||
|---|---|---|---|---|---|
| OR值(95%CI) | P值 | OR值(95%CI) | P值 | ||
| Q1 | 38 | 27.187(10.632~69.519) | < 0.001 | 28.150(10.651~74.398) | < 0.001 |
| Q2 | 48 | 5.639(2.602~12.222) | < 0.001 | 5.737(2.579~12.759) | < 0.001 |
| Q3 | 59 | 2.472(1.127~5.420) | 0.024 | 2.603(1.162~5.834) | 0.020 |
| Q4 | 132 | 1.0 | - | 1.0 | - |
| 趋势性检验P值 | <0.001 | <0.001 | |||
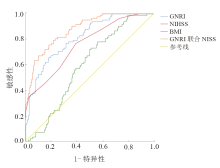
图1
GNRI、NIHSS、BMI和GNRI联合NIHSS预测神经功能的ROC曲线"

表4
GNRI、NIHSS、BMI和GNRI联合NIHSS预测神经功能预后的ROC统计值"
| 指标 | AUC(95%CI) | Z值 | P值 | Youden指数 | 最佳截断值 | 敏感性/% | 特异性/% |
|---|---|---|---|---|---|---|---|
| GNRI | 0.812(0.761~0.856) | 11.576 | < 0.001 | 0.4739 | 92.69 | 65.85 | 81.54 |
| NIHSS | 0.759(0.704~0.808) | 8.328 | < 0.001 | 0.3734 | 11.00 | 76.83 | 60.51 |
| BMI | 0.594(0.533~0.652) | 2.716 | 0.007 | 0.2189 | 23.81 | 73.17 | 48.72 |
| GNRI联合NIHSS | 0.875(0.830~0.912) | 17.389 | < 0.001 | 0.5722 | 0.277 | 79.21 | 82.95 |
| [1] |
SABBOUH T, TORBEY M T. Malnutrition in stroke patients: risk factors, assessment, and management[J]. Neurocrit Care, 2018, 29(3): 374-384.
doi: 10.1007/s12028-017-0436-1 pmid: 28799021 |
| [2] |
YUAN K, ZHU S, WANG H, et al. Association between malnutrition and long-term mortality in older adults with ischemic stroke[J]. Clin Nutr, 2021, 40(5): 2535-2542.
doi: 10.1016/j.clnu.2021.04.018 pmid: 33932800 |
| [3] |
HAO R, QI X, XIA X, et al. Malnutrition on admission increases the in-hospital mortality and length of stay in elder adults with acute ischemic stroke[J]. J Clin Lab Anal, 2022, 36(1): e24132.
doi: 10.1002/jcla.v36.1 |
| [4] | 四川大学华西循证护理中心, 中华护理学会护理管理专业委员会, 中华医学会神经外科学分会. 中国卒中肠内营养护理指南[J]. 中国循证医学杂志, 2021, 21(6): 628-641. |
| Evidence-based Nursing Center of West China Hospital of Sichuan University, Nursing Management Professional Committee of Chinese Nursing Association, Chinese Neurosurgical Society. Nursing practice guideline for enteral nutrition in patients with stroke[J]. Chin J Evid-Based Med, 2021, 21(6): 628-641. | |
| [5] | 中国卒中营养标准化管理专家委员会. 中国卒中营养标准化管理专家共识[J]. 中国卒中杂志, 2020, 15(6): 681-689. |
| Chinese Stroke Nutrition Standardization Management Expert Committee. Expert consensus on standardized management of stroke nutrition in China[J]. Chin J Stroke, 2020, 15(6): 681-689. | |
| [6] |
BURGOS R, BRETÓN I, CEREDA E, et al. ESPEN guideline clinical nutrition in neurology[J]. Clin Nutr, 2018, 37(1): 354-396.
doi: S0261-5614(17)30318-7 pmid: 29274834 |
| [7] |
BOUILLANNE O, MORINEAU G, DUPONT C, et al. Geriatric Nutritional Risk Index: a new index for evaluating at-risk elderly medical patients[J]. Am J Clin Nutr, 2005, 82(4): 777-783.
doi: 10.1093/ajcn/82.4.777 pmid: 16210706 |
| [8] |
NAKAGAWA N, MARUYAMA K, HASEBE N. Utility of Geriatric Nutritional Risk Index in patients with chronic kidney disease: a mini-review[J]. Nutrients, 2021, 13(11): 3688.
doi: 10.3390/nu13113688 |
| [9] |
LIU H T, WU S C, TSAI C H, et al. Association between Geriatric Nutritional Risk Index and mortality in older trauma patients in the intensive care unit[J]. Nutrients, 2020, 12(12): 3861-3870.
doi: 10.3390/nu12123861 |
| [10] |
SHEN F, MA Y, GUO W, et al. Prognostic value of Geriatric Nutritional Risk Index for patients with non-small cell lung cancer: a systematic review and meta-analysis[J]. Lung, 2022, 200(5): 661-669.
doi: 10.1007/s00408-022-00567-6 pmid: 36114300 |
| [11] |
XU J, ZHOU X, ZHENG C. The Geriatric Nutritional Risk Index independently predicts adverse outcomes in patients with pyogenic liver abscess[J]. BMC Geriatr, 2019, 19(1): 14.
doi: 10.1186/s12877-019-1030-5 pmid: 30651062 |
| [12] |
ZHU L, XIA J, SHAO X, et al. The relationship between the baseline Geriatric Nutritional Risk Index (GNRI) and neurological function at the convalescence stage in patients with stroke: a cross-sectional study[J]. BMC Geriatr, 2023, 23(1): 173.
doi: 10.1186/s12877-023-03919-w pmid: 36973674 |
| [13] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国各类主要脑血管病诊断要点2019[J]. 中华神经科杂志, 2019, 52(9): 710-715. |
| [14] |
KWAH L K, DIONG J. National Institutes of Health Stroke Scale (NIHSS)[J]. J Physiother, 2014, 60(1): 61.
doi: 10.1016/j.jphys.2013.12.012 pmid: 24856948 |
| [15] |
BAMFORD J, SANDERCOCK P, DENNIS M, et al. Classification and natural history of clinically identifiable subtypes of cerebral infarction[J]. Lancet, 1991, 337(8756): 1521-1526.
doi: 10.1016/0140-6736(91)93206-o pmid: 1675378 |
| [16] |
BANKS J L, MAROTTA C A. Outcomes validity and reliability of the modified Rankin Scale: implications for stroke clinical trials: a literature review and synthesis[J]. Stroke, 2007, 38(3): 1091-1096.
doi: 10.1161/01.STR.0000258355.23810.c6 pmid: 17272767 |
| [17] |
ZHANG M, YE S, HUANG X, et al. Comparing the prognostic significance of nutritional screening tools and ESPEN-DCM on 3-month and 12-month outcomes in stroke patients[J]. Clin Nutr, 2021, 40(5): 3346-3353.
doi: 10.1016/j.clnu.2020.11.001 pmid: 33221053 |
| [18] |
WANG L, ZHANG D, XU J. Association between the Geriatric Nutritional Risk Index, bone mineral density and osteoporosis in type 2 diabetes patients[J]. J Diabetes Investig, 2020, 11(4): 956-963.
doi: 10.1111/jdi.v11.4 |
| [19] |
CARLOS S A, LORENZO L M, JOSE P F, et al. Malnutrition screening and assessment[J]. Nutrients, 2022, 14(12): 2392.
doi: 10.3390/nu14122392 |
| [20] |
CORISH C A, BARDON L A. Malnutrition in older adults: screening and determinants[J]. Proc Nutr Soc, 2019, 78(3): 372-379.
doi: 10.1017/S0029665118002628 pmid: 30501651 |
| [21] |
GÜÇ Z G, ALACACIOĞLU A, KALENDER M E, et al. HALP score and GNRI: Simple and easily accessible indexes for predicting prognosis in advanced stage NSCLC patients. The İzmir oncology group (IZOG) study[J]. Front Nutr, 2022, 9: 905292.
doi: 10.3389/fnut.2022.905292 |
| [22] |
LI H, CEN K, SUN W, et al. Prognostic value of Geriatric Nutritional Risk Index in elderly patients with heart failure: a meta-analysis[J]. Aging Clin Exp Res, 2021, 33(6): 1477-1486.
doi: 10.1007/s40520-020-01656-3 |
| [23] |
SUGIYAMA Y, NAIKI T, TASAKI Y, et al. GNRI sustainability during one cycle of first-line chemotherapy as a prognostic indicator in patients with metastatic urothelial carcinoma[J]. Oncology, 2023, 101(4): 224-233.
doi: 10.1159/000529203 |
| [24] |
CEREDA E, PEDROLLI C. The Geriatric Nutritional Risk Index[J]. Curr Opin Clin Nutr Metab Care, 2009, 12(1): 1-7.
doi: 10.1097/MCO.0b013e3283186f59 |
| [25] | 范玉华, 姬晓昙, 蓝琳芳. 国内脑卒中临床试验疗效判断方法中改良Rankin评分的应用现状[J]. 中国神经精神疾病杂志, 2015, 41(7): 412-415. |
| FAN Y H, JI X T, LAN L F. The application of mRS in the methods of outcome assessment in Chinese stroke trials[J]. Chin J Nerv Mental Dis, 2015, 41(7): 412-415. | |
| [26] | 姜逍瑶, 赵旭东, 鲍磊, 等. 老年营养风险指数对急性缺血性脑卒中患者预后的预测价值[J]. 中华老年心脑血管病杂志, 2023, 25(1): 35-38. |
| JIANG X Y, ZHAO X D, BAO L, et al. Prognostic value of Geriatric Nutritional Risk Index in patients with acute ischemic stroke[J]. Chin J Geriatr Heart Brain Vessel Dis, 2023, 25(1): 35-38. | |
| [27] |
KAZI S A, SIDDIQUI M, MAJID S. Stroke outcome prediction using admission nihss in anterior and posterior circulation stroke[J]. J Ayub Med Coll Abbottabad, 2021, 33(2): 274-278.
pmid: 34137544 |
| [28] |
CHOI V, KATE M, KOSIOR J C, et al. National Institutes of Health Stroke Scale score is an unreliable predictor of perfusion deficits in acute stroke[J]. Int J Stroke, 2015, 10(4): 582-588.
doi: 10.1111/ijs.12438 pmid: 25845906 |
| [29] |
OLIVATO S, NIZZOLI S, CAVAZZUTI M, et al. e-NIHSS: an expanded national institutes of health stroke scale weighted for anterior and posterior circulation strokes[J]. J Stroke Cerebrovasc Dis, 2016, 25(12): 2953-2957.
doi: S1052-3057(16)30283-X pmid: 27693107 |
| [30] |
QUAN H, CHEN X, LUO J, et al. A generalized weighted combination test of treatment effect for clinical trials with a sequential parallel comparison design and binary endpoint[J]. Stat Med, 2022, 41(15): 2725-2744.
doi: 10.1002/sim.v41.15 |
| [31] |
NISHIOKA S, OMAGARI K, NISHIOKA E, et al. Concurrent and predictive validity of the Mini Nutritional Assessment Short-Form and the Geriatric Nutritional Risk Index in older stroke rehabilitation patients[J]. J Hum Nutr Diet, 2020, 33(1): 12-22.
doi: 10.1111/jhn.12699 pmid: 31435986 |
| [32] |
JENSEN G L, CEDERHOLM T, CORREIA M, et al. GLIM criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community[J]. JPEN J Parenter Enteral Nutr, 2019, 43(1): 32-40.
doi: 10.1002/jpen.1440 pmid: 30175461 |
| [33] |
POHL M, HESSZENBERGER D, KAPUS K, et al. Ischemic stroke mimics: a comprehensive review[J]. J Clin Neurosci, 2021, 93: 174-182.
doi: 10.1016/j.jocn.2021.09.025 pmid: 34656244 |
| [34] |
ZIELIŃSKA-NOWAK E, CICHON N, SALUK-BIJAK J, et al. Nutritional supplements and neuroprotective diets and their potential clinical significance in post-stroke rehabilitation[J]. Nutrients, 2021, 13(8): 2704.
doi: 10.3390/nu13082704 |
| [35] |
MURRELL J E, PISEGNA J L, JUCKETT L A. Implementation strategies and outcomes for occupational therapy in adult stroke rehabilitation: a scoping review[J]. Implement Sci, 2021, 16(1): 105.
doi: 10.1186/s13012-021-01178-0 pmid: 34922568 |
| [36] |
GASBARRINO K, DI IORIO D, DASKALOPOULOU S S. Importance of sex and gender in ischaemic stroke and carotid atherosclerotic disease[J]. Eur Heart J, 2022, 43(6): 460-473.
doi: 10.1093/eurheartj/ehab756 |
| [1] | 王航宇, 葛可可, 范永红, 都丽露, 邹敏, 封磊. 基于ICD-11和ICF主动式音乐疗法改善认知障碍老年人认知功能的系统综述[J]. 《中国康复理论与实践》, 2024, 30(1): 36-43. |
| [2] | 葛可可, 范永红, 王航宇, 都丽露, 李长江, 邹敏. 失眠老年人正念干预健康效益的系统综述[J]. 《中国康复理论与实践》, 2024, 30(1): 54-60. |
| [3] | 林娜, 高菡璐, 卢惠苹, 陈燕清, 郑军凡, 陈述荣. 虚拟现实技术对脑卒中上肢功能影响的弥散张量成像研究[J]. 《中国康复理论与实践》, 2024, 30(1): 61-67. |
| [4] | 王昊懿, 史亚伟, 鲁俊, 许光旭. 主观垂直感知障碍对脑卒中患者功能影响的回顾性研究[J]. 《中国康复理论与实践》, 2024, 30(1): 68-73. |
| [5] | 陈珺雯, 陈谦, 陈程, 李淑月, 刘玲玲, 吴存书, 龚翔, 鲁俊, 许光旭. 改良八段锦身体活动对脑卒中患者心肺功能、运动功能和日常生活活动能力的效果[J]. 《中国康复理论与实践》, 2024, 30(1): 74-80. |
| [6] | 胡永林, 马颖, 窦超, 陆安民, 江小鸽, 宋新建, 肖玉华. 肩部控制训练联合神经松动术对脑卒中偏瘫患者肩痛及上肢功能的效果[J]. 《中国康复理论与实践》, 2024, 30(1): 81-86. |
| [7] | 王贺, 韩靓, 阚梦凡, 于少泓. 电刺激治疗脑卒中后肩手综合征有效性的系统评价与Meta分析[J]. 《中国康复理论与实践》, 2023, 29(9): 1048-1056. |
| [8] | 杨雅楠, 穆丽萍, 邢凤梅, 薛新宏, 王晓光, 陶徉聿, 孙竹梅, 张小丽. 基于计划行为理论的干预对肌少症老年人肌肉衰减状况及平衡能力的效果[J]. 《中国康复理论与实践》, 2023, 29(8): 869-874. |
| [9] | 孙藤方, 任梦婷, 杨琳, 王耀霆, 王红雨, 闫兴洲. 高压氧治疗联合重复外周磁刺激干预脑卒中患者踝运动功能和平衡能力的效果[J]. 《中国康复理论与实践》, 2023, 29(8): 875-881. |
| [10] | 王亚楠, 刘西花. 脑卒中偏瘫患者主观和客观平衡功能测量的相关性及预测效能[J]. 《中国康复理论与实践》, 2023, 29(8): 890-895. |
| [11] | 蒋长好, 黄辰, 高晓妍, 戴元富, 赵国明. 神经反馈训练对老年人认知功能效果的系统综述[J]. 《中国康复理论与实践》, 2023, 29(8): 903-909. |
| [12] | 王海云, 王寅, 周信杰, 何爱群. 基于“中枢-外周-中枢”理论的经颅直流电刺激结合针刺干预脑卒中患者中枢及上肢功能的效果[J]. 《中国康复理论与实践》, 2023, 29(8): 919-925. |
| [13] | 陈怡婷, 王倩, 崔慎红, 李映彩, 张思鈺, 魏衍旭, 任慧, 冷军, 陈斌. 双侧序贯重复经颅磁刺激干预脑卒中患者上肢运动功能的效果[J]. 《中国康复理论与实践》, 2023, 29(8): 926-932. |
| [14] | 李振亚, 孙洁, 郭鹏飞, 王光明. 脑卒中患者口期和咽期吞咽功能改变与误吸的相关性:基于电视透视吞咽检查[J]. 《中国康复理论与实践》, 2023, 29(8): 933-939. |
| [15] | 华玲, 张一楠, 郑玉, 孙俏仪, 房辉, 宋达. 手控节律音乐治疗对脑卒中后单侧空间忽略的效果[J]. 《中国康复理论与实践》, 2023, 29(7): 833-838. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
|
||