


《中国康复理论与实践》 ›› 2025, Vol. 31 ›› Issue (12): 1414-1420.doi: 10.3969/j.issn.1006-9771.2025.12.005
薛蕾( )
)
收稿日期:2025-05-22
修回日期:2025-10-11
出版日期:2025-12-25
发布日期:2025-12-29
通讯作者:
薛蕾
E-mail:xiaoxiaogu321@163.com
作者简介:薛蕾(1985-),女,汉族,北京市人,护师,主要从事心内科护理、导管介入。
XUE Lei()
Received:2025-05-22
Revised:2025-10-11
Published:2025-12-25
Online:2025-12-29
Contact:
XUE Lei
E-mail:xiaoxiaogu321@163.com
摘要:
目的 调查经皮冠状动脉介入术(PCI)后患者Ⅰ期心脏康复运动时长现状,并分析其影响因素。
方法 回顾分析2022年5月至2024年5月行PCI且术后参与Ⅰ期心脏康复患者120例,采用自制调查表收集临床资料,记录心脏康复运动时长。
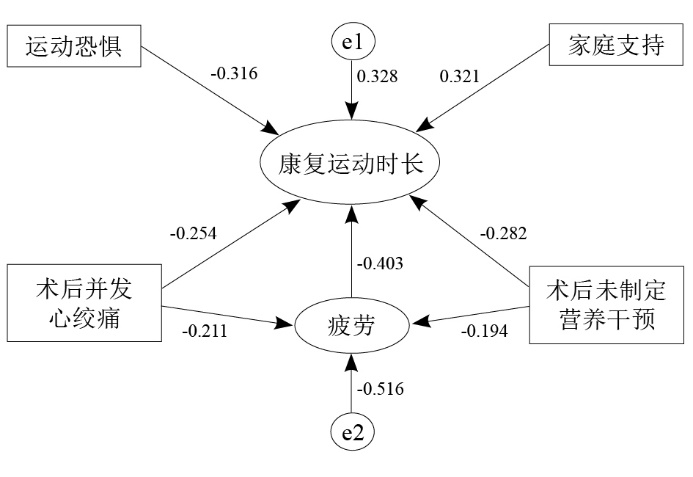
结果 心脏康复运动时长为每天(19.45±6.32) min,疲劳(62.55±4.37)分,家庭支持(84.87±10.65)分,运动恐惧(41.98±5.24)分;不同年龄、体质量、心功能分级、术后是否并发心绞痛、术后制定营养干预的患者,康复运动时长有显著性差异(P < 0.05)。Pearson相关性分析显示,康复运动时长与疲劳(r = -0.247, P < 0.05)、运动恐惧(r = -0.235, P < 0.05)、家庭支持(r = 0.206, P < 0.05)相关。多元线性回归分析显示,术后并发心绞痛(B = -3.210, 95%CI -5.564~-0.855)、术后制定营养干预(B = -3.738, 95%CI -6.790~-0.686)、疲劳(B = -0.182, 95%CI -0.349~-0.014)、家庭支持(B = 0.086, 95%CI 0.003~0.169)、运动恐惧(B = -0.139, 95%CI -0.248~-0.030)均是康复运动时长的独立影响因素(P < 0.05)。结构方程显示,5个独立影响因素对康复运动时长均有直接效应,术后并发心绞痛和术后制定营养干预还有间接效应。
结论 PCI术后患者Ⅰ期心脏康复运动时长有待提高,患者术后并发心绞痛、未制定营养干预、疲劳、运动恐惧以及家庭支持不足均会影响康复运动时长,应采取针对性干预,促进患者术后恢复。
中图分类号:
薛蕾. 经皮冠状动脉介入术后患者Ⅰ期心脏康复运动时长的影响因素[J]. 《中国康复理论与实践》, 2025, 31(12): 1414-1420.
XUE Lei. Factors relating with exercise duration of phase I cardiac rehabilitation for patients after percutaneous coronary intervention[J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(12): 1414-1420.
表1
患者各项评定结果(n = 120)"
| 项目 | 条目数 | 维度均分 | 条目均分 |
|---|---|---|---|
| 疲劳总分 | 20 | 62.55±4.37 | 3.21±0.28 |
| 体力疲劳 | 10 | 30.74±2.18 | 3.06±0.32 |
| 脑力疲劳 | 4 | 12.32±1.96 | 2.98±1.11 |
| 动力下降 | 3 | 9.63±1.21 | 3.17±0.33 |
| 活动减少 | 3 | 9.45±1.88 | 3.15±0.46 |
| 家庭支持总分 | 30 | 84.87±10.65 | 2.83±0.36 |
| 亲密度 | 16 | 45.31±5.28 | 2.81±0.47 |
| 适应度 | 14 | 39.65±6.47 | 2.83±0.46 |
| 运动恐惧总分 | 17 | 41.98±5.24 | 2.47±0.31 |
| 危险感知 | 4 | 9.91±1.23 | 2.51±0.33 |
| 运动恐惧 | 4 | 9.87±1.30 | 2.51±0.29 |
| 运动回避 | 5 | 12.56±1.77 | 2.67±0.58 |
| 功能紊乱 | 4 | 10.23±1.42 | 2.54±0.36 |
表2
不同特征患者康复运动时长比较"
| 特征 | n | 康复运动时长/(min·d-1) | t/F值 | P值 | |
|---|---|---|---|---|---|
| 年龄 | < 60岁 | 57 | 19.68±6.24 | 2.178 | 0.031 |
| ≥ 60岁 | 63 | 17.41±5.17 | |||
| 性别 | 男 | 66 | 19.24±6.08 | 0.063 | 0.950 |
| 女 | 54 | 19.31±5.99 | |||
| 住院时间 | ≤ 1周 | 78 | 19.21±5.86 | 1.795 | 0.075 |
| > 1周 | 42 | 17.42±3.69 | |||
| 病程 | < 5年 | 84 | 19.34±6.27 | 0.064 | 0.949 |
| ≥ 5年 | 36 | 19.26±6.35 | |||
| 体质量 | 偏瘦 | 15 | 15.54±4.27 | 3.962 | 0.022 |
| 正常 | 87 | 19.51±6.86 | |||
| 超重/肥胖 | 18 | 16.11±5.24 | |||
| NYHA心功能分级 | ≤ Ⅱ级 | 98 | 19.51±6.68 | 2.773 | 0.007 |
| > Ⅱ级 | 22 | 15.36±4.47 | |||
| 受教育程度 | 高中及以下 | 15 | 19.42±6.25 | 0.012 | 0.987 |
| 专科 | 47 | 19.39±6.31 | |||
| 本科及以上 | 58 | 19.40±6.27 | |||
| 家庭人均月收入 | < 3000元 | 14 | 19.44±6.33 | 0.012 | 0.988 |
| 3000~8000元 | 64 | 19.21±6.38 | |||
| > 8000元 | 42 | 19.37±6.42 | |||
| 职业 | 在职 | 37 | 19.35±6.38 | 0.001 | 0.999 |
| 无业/自由职业 | 31 | 19.41±6.27 | |||
| 退休 | 52 | 19.39±6.30 | |||
| 术后并发心绞痛 | 有 | 24 | 16.32±4.65 | 2.131 | 0.035 |
| 无 | 96 | 19.27±6.36 | |||
| 术后制定营养干预 | 有 | 68 | 19.59±6.21 | 1.991 | 0.049 |
| 无 | 52 | 17.54±4.65 | |||
表3
康复运动时长与疲劳、家庭支持、运动恐惧的相关性"
| 因素 | n | r | SE | P | 95%置信区间 | |
|---|---|---|---|---|---|---|
| 下限 | 上限 | |||||
| 疲劳 | 120 | -0.247 | 0.075 | 0.007 | -0.393 | -0.094 |
| 家庭支持 | 120 | 0.206 | 0.087 | 0.024 | 0.040 | 0.379 |
| 运动恐惧 | 120 | -0.235 | 0.086 | 0.010 | -0.411 | -0.065 |
表4
赋值方法"
| 变量 | 赋值 |
|---|---|
| 年龄 | < 60岁 = 0,≥ 60岁 = 1 |
| 体质量 | 正常 = 0,偏瘦/超重/肥胖 = 1 |
| NYHA心功能分级 | ≤ Ⅱ级 = 0,> Ⅱ级 = 1 |
| 术后并发心绞痛 | 无 = 0,有 = 1 |
| 术后制定营养干预 | 有 = 0,无 = 1 |
| 疲劳 | 原值 |
| 家庭支持 | 原值 |
| 运动恐惧 | 原值 |
表5
康复运动时长的影响因素"
| 变量 | 未标准化系数 | β值 | t值 | P值 | 95%置信区间 | 共线性检验 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | 下限 | 上限 | 容差 | VIF | |||||
| 常量 | 16.581 | 3.696 | - | 2.541 | 0.012 | 4.975 | 26.188 | - | - | |
| 年龄 | -1.107 | 0.100 | -0.111 | -1.071 | 0.286 | -0.306 | 0.091 | 0.732 | 1.710 | |
| 体质量 | -1.090 | 1.627 | -0.095 | -0.670 | 0.504 | -4.313 | 2.132 | 0.391 | 2.556 | |
| NYHA心功能分级 | 0.081 | 1.549 | 0.003 | 0.031 | 0.975 | -3.052 | 3.116 | 0.662 | 1.510 | |
| 术后并发心绞痛 | -3.210 | 1.189 | -0.281 | -2.700 | 0.008 | -5.564 | -0.855 | 0.699 | 1.430 | |
| 术后制定营养干预 | -3.738 | 1.541 | -0.325 | -2.425 | 0.017 | -6.790 | -0.686 | 0.440 | 2.275 | |
| 疲劳 | -0.182 | 0.085 | -0.223 | -2.152 | 0.034 | -0.349 | -0.014 | 0.724 | 1.382 | |
| 家庭支持 | 0.086 | 0.042 | 0.205 | 2.041 | 0.043 | 0.003 | 0.169 | 0.792 | 1.263 | |
| 运动恐惧 | -0.139 | 0.055 | -0.237 | -2.524 | 0.013 | -0.248 | -0.030 | 0.865 | 1.156 | |
表6
结构方程模型主要拟合指标"
| 模型拟合指标 | 测定值 | 适配标准 |
|---|---|---|
| 卡方自由度比 | 2.146 | ≤ 3.00 |
| 渐进残差均方根 | 0.002 | ≤ 0.08 |
| 非规准适配指数 | 0.961 | ≥ 0.90 |
| 增值拟合指数 | 0.934 | ≥ 0.90 |
| 拟合优度指数 | 0.952 | ≥ 0.90 |
| 调整后拟合优度指数 | 0.933 | ≥ 0.90 |
表7
康复运动时长影响因素的路径分析(效应值)"
| 项目 | 直接效应 | 间接效应 | 总效应 |
|---|---|---|---|
| 术后并发心绞痛 | -0.254 | -0.085 | -0.339 |
| 术后未制定营养干预 | -0.282 | -0.065 | -0.347 |
| 疲劳 | -0.403 | - | -0.403 |
| 家庭支持 | 0.321 | - | 0.321 |
| 运动恐惧 | -0.316 | - | -0.316 |
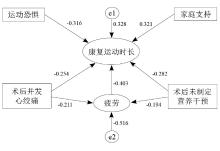
图1
康复运动时长影响因素的路径分析"
| [1] | 刘明波, 何新叶, 杨晓红, 等. «中国心血管健康与疾病报告2023»要点解读[J]. 中国心血管杂志, 2024, 29(4): 305-324. |
| LIU M B, HE X Y, YANG X H, et al. Interpretation of Report on Cardiovascular Health and Diseases in China 2023[J]. Chin J Cardiovasc Med, 2024, 29(4): 305-324. | |
| [2] |
AKBARI T, AL-LAMEE R. Percutaneous coronary intervention in multi-vessel disease[J]. Cardiovasc Revasc Med, 2022, 44: 80-91.
doi: 10.1016/j.carrev.2022.06.254 |
| [3] |
HOOLE S P, BAMBROUGH P. Recent advances in percutaneous coronary intervention[J]. Heart, 2020, 106(18): 1380-1386.
doi: 10.1136/heartjnl-2019-315707 pmid: 32522821 |
| [4] | KUMAR A, JNEID H. Predicting mortality after percutaneous coronary intervention: the need for improved risk models[J]. Catheter Cardiovasc Interv, 2021, 98(7): 1298-1299. |
| [5] | DIBBEN G, FAULKNER J, OLDRIDGE N, et al. Exercise-based cardiac rehabilitation for coronary heart disease[J]. Cochrane Database Syst Rev, 2021, 11(11): CD001800. |
| [6] |
毛越, 徐剑锋, 李梅, 等. 经导管主动脉瓣置换术患者Ⅰ期心脏康复的最佳证据应用[J]. 中华护理杂志, 2022, 57(5): 563-569.
doi: 10.3761/j.issn.0254-1769.2022.05.008 |
|
MAO Y, XU J F, LI M, et al. Best evidence application of phase Ⅰ cardiac rehabilitation in transcatheter aortic valve replacement patients[J]. Chin J Nurs, 2022, 57(5): 563-569.
doi: 10.3761/j.issn.0254-1769.2022.05.008 |
|
| [7] |
ZHANG M, JIN A, ZHOU X, et al. A quasi-experimental study on couple-based exercise program improving cardiac rehabilitation exercise compliance in post-PCI patients[J]. BMC Cardiovasc Disord, 2024, 24(1): 640.
doi: 10.1186/s12872-024-04282-3 |
| [8] | 中国医师协会心血管内科医师分会. 心血管疾病防治指南和共识2014[M]. 北京: 人民卫生出版社, 2014: 37-143. |
| Chinese College of Cardiology Physicians, Chinese Medical Doctor Association. Guidelines and consensuses for prevention and treatment of cardiovascular diseases 2014[M]. Beijing: People's Medical Publishing House, 2014: 37-143. | |
| [9] | 韩雅玲. 中国经皮冠状动脉介入治疗指南(2016)解读[J]. 中国循环杂志, 2016, 31(S2): 5-8. |
| HAN Y L. Interpretation of Chinese Guidelines for Percutaneous Coronary Intervention (2016)[J]. Chin Circ J, 2016, 31(S2): 5-8. | |
| [10] | 张海洪, 丛亚丽. 世界医学会«赫尔辛基宣言»2024版修订述评[J]. 医学与哲学, 2024, 45(21): 18-23. |
| ZHANG H H, CONG Y L. A review of the 2024 revision of the World Medical Association Declaration of Helsinki[J]. Med Philos, 2024, 45(21): 18-23. | |
| [11] | 李红娟, 杨柳, 张楠. 身体质量指数作为肥胖筛查标准的判别准确性评价[J]. 中国预防医学杂志, 2014, 15(6): 571-575. |
| LI H J, YANG L, ZHANG N. Accuracy of body mass index as a screening standard for obesity[J]. Chin J Prev Med, 2014, 15(6): 571-575. | |
| [12] | 曹楚雄, 朱文艺, 白倩, 等. 冠心病PCI病人围手术期营养治疗效果及临床结局的评价研究[J]. 肠外与肠内营养, 2023, 30(2): 75-79, 84. |
| CAO C X, ZHU W Y, BAI Q, et al. Evaluation of perioperative nutritional therapy effect and clinical outcome of PCI patients with coronary heart disease[J]. Parenter Enteral Nutr, 2023, 30(2): 75-79, 84. | |
| [13] | 陈桂铃, 严凤娇, 张婉, 等. 重症心脏疾病患者Ⅰ期心脏康复运动时长现况及其影响因素分析[J]. 现代临床护理, 2022, 21(9): 8-12. |
| CHEN G L, YAN F J, ZHANG W, et al. Duration of cardiac rehabilitation exercise and its influencing factors in severe CCU patients[J]. Mod Clin Nurs, 2022, 21(9): 8-12. | |
| [14] | 苗雨, 刘晓虹, 刘伟志, 等. 多维疲劳量表中文版在军队基层医护人员中的初步修订[J]. 中国心理卫生杂志, 2008, 22(9): 658-660, 668. |
| MIAO Y, LIU X H, LIU W Z, et al. Initial revision of the Chinese Version of Multidimensional Fatigue Inventory-20 in medical staff of military basic level[J]. Chin Ment Health J, 2008, 22(9): 658-660, 668. | |
| [15] | 张赛, 路孝琴, 杜蕾, 等. 家庭功能评价工具家庭亲密度和适应性量表的发展及其应用研究[J]. 中国全科医学, 2010, 13(7): 725-728. |
| ZHANG S, LU X Q, DU L, et al. Development and application of FACES[J]. Chin Gen Pract, 2010, 13(7): 725-728. | |
| [16] |
WEERMEIJER J D, MEULDERS A. Clinimetrics: Tampa scale for kinesiophobia[J]. J Physiother, 2018, 64(2): 126.
doi: S1836-9553(18)30002-X pmid: 29567379 |
| [17] |
WU L, LI J, CHEN L, et al. The efficacy and safety of phase I cardiac rehabilitation in patients hospitalized in cardiac intensive care unit with acute decompensated heart failure: a study protocol for a randomized, controlled, clinical trial[J]. Front Cardiovasc Med, 2022, 9: 788503.
doi: 10.3389/fcvm.2022.788503 |
| [18] |
WANG Y, XIAO Y, TANG J, et al. Effects of early phase 1 cardiac rehabilitation on cardiac function evaluated by impedance cardiography in patients with coronary heart disease and acute heart failure[J]. Front Cardiovasc Med, 2022, 9: 958895.
doi: 10.3389/fcvm.2022.958895 |
| [19] | 中华医学会, 中华医学会杂志社, 中华医学会全科医学分会, 等. 冠心病心脏康复基层指南(2020年)[J]. 中华全科医师杂志, 2021, 20(2): 150-165. |
| Chinese Medical Association, Chinese Medical Association Journal, General Practice Branch of Chinese Medical Association, et al. Guideline for primary care of cardiac rehabilitation of coronary artery disease (2020)[J]. Chin J Gen Pract, 2021, 20(2): 150-165. | |
| [20] | 严凤娇, 宋文馨, 陈桂铃, 等. 急诊经皮冠状动脉介入术后患者Ⅰ期心脏康复方案实施完成度及其影响因素分析[J]. 中国护理管理, 2021, 21(11): 1617-1621. |
| YAN F J, SONG W X, CHEN G L, et al. The completion rate of phase Ⅰ cardiac rehabilitation program and influencing factors of emergency PCI patients[J]. Chin Nurs Manag, 2021, 21(11): 1617-1621. | |
| [21] |
SUN T, MA M, HUANG X, et al. Prognostic impacts of geriatric nutritional risk index in patients with ischemic heart failure after percutaneous coronary intervention[J]. Clin Nutr, 2023, 42(8): 1260-1267.
doi: 10.1016/j.clnu.2023.05.023 pmid: 37343410 |
| [22] |
QIN J, XIONG J, WANG X, et al. Kinesiophobia and its association with fatigue in CHF patients[J]. Clin Nurs Res, 2022, 31(7): 1316-1324.
doi: 10.1177/10547738221081230 |
| [23] |
WANG Q, DU N. Relationship between kinesiophobia and quality of life among patients with breast cancer-related lymphedema: chain-mediating effect of self-care and functional exercise compliance[J]. Asia Pac J Oncol Nurs, 2023, 11(1): 100346.
doi: 10.1016/j.apjon.2023.100346 |
| [24] |
NGUYEN A P, MAI L A T, SPIES L A, et al. Interventions for family support in cardiometabolic disease: an integrative review[J]. Nurs Open, 2023, 10(9): 5797-5812.
doi: 10.1002/nop2.v10.9 |
| [25] |
FELDMAN E C H, DURKIN L K, GREENLEY R N. Family support is associated with fewer adherence barriers and greater intent to adhere to oral medications in pediatric IBD[J]. J Pediatr Nurs, 2021, 60: 58-64.
doi: 10.1016/j.pedn.2021.01.026 pmid: 33618177 |
| [26] | 梁晓慧, 谷文婷, 王晓华, 等. 老年冠心病患者心脏康复运动依从性调查及影响因素分析[J]. 老年医学与保健, 2024, 30(2): 320-324, 342. |
| LIANG X H, GU W T, WANG X H, et al. Investigation of compliance with cardiac rehabilitation exercise in elderly patients with coronary heart disease and analysis of its influencing factors[J]. Geriatr Health Care, 2024, 30(2): 320-324, 342. | |
| [27] |
OLAGBEMIDE O J, OMOSANYA O E, AYODAPO A O, et al. Family support and medication adherence among adult type 2 diabetes: any meeting point?[J]. Ann Afr Med, 2021, 20(4): 282-287.
doi: 10.4103/aam.aam_62_20 pmid: 34893566 |
| [28] |
FORD T J, BERRY C. Angina: contemporary diagnosis and management[J]. Heart, 2020, 106(5): 387-398.
doi: 10.1136/heartjnl-2018-314661 pmid: 32054665 |
| [29] |
MEDINA-INOJOSA J R, GRACE S L, SUPERVIA M, et al. Dose of cardiac rehabilitation to reduce mortality and morbidity: a population-based study[J]. J Am Heart Assoc, 2021, 10(20): e021356.
doi: 10.1161/JAHA.120.021356 |
| [30] | DOWNER S, BERKOWITZ S A, HARLAN T S, et al. Food is medicine: actions to integrate food and nutrition into healthcare[J]. BMJ, 2020, 369: m2482. |
| [31] |
GUERRA-SÁNCHEZ L, FRESNO-FLORES M, MARTÍNEZ-RINCÓN C. Effect of a double nutritional intervention on the nutritional status, functional capacity, and quality of life of patients with chronic heart failure: 12-month results from a randomized clinical trial[J]. Nutr Hosp, 2020, 34(3): 422-431.
doi: 10.20960/nh.250 |
| [32] |
SONG G, WANG X, WEI C, et al. The complex inflammatory and nutritional indices to predict prognostic risk for patients with acute coronary syndrome undergoing percutaneous coronary intervention[J]. Immun Inflamm Dis, 2025, 13(3): e70180.
doi: 10.1002/iid3.v13.3 |
| [33] |
KANDA D, IKEDA Y, TAKUMI T, et al. Impact of nutritional status on prognosis in acute myocardial infarction patients undergoing percutaneous coronary intervention[J]. BMC Cardiovasc Disord, 2022, 22(1): 3.
doi: 10.1186/s12872-021-02448-x |
| [1] | 解海霞, 胡心星, 翟华, 林佩佩, 何建辉, 张佳, 董晓婉, 苌凤水. 生活重建训练对慢性期脊髓损伤患者及其照顾者焦虑和抑郁的效果[J]. 《中国康复理论与实践》, 2025, 31(11): 1333-1341. |
| [2] | 刘晨, 董理权, 闫媚, 江华. 功能障碍人群辅助器具适配度评价及影响因素分析[J]. 《中国康复理论与实践》, 2025, 31(11): 1354-1364. |
| [3] | 陈盼盼, 王炳龙, 董理权, 刘夕东, 杨幼平, 李佳玥. 成都肢体残疾人未满足辅助技术需求及其相关因素[J]. 《中国康复理论与实践》, 2024, 30(5): 598-605. |
| [4] | 蒋娜, 卫宁, 曾艳玲, 张倩, 益筱哲, 陈万强, 景玉珍, 寄婧, 郭旭升, 裴泓波, 王建云. 康复患者次均住院费用影响因素的分析:基于分位数回归模型[J]. 《中国康复理论与实践》, 2024, 30(4): 397-403. |
| [5] | 王子豪, 李昕华, 蒋慧萍, 郭赛男, 梁秋曼, 史婷奇. 全膝关节置换术后短期膝关节功能及其影响因素[J]. 《中国康复理论与实践》, 2024, 30(1): 111-118. |
| [6] | 王光程, 段明雪, 郭桐桐, 邢洋, 董志伟, 张琳琳, 郭培武, 井淇, 郑文贵. 康复治疗师职业发展及其转型影响因素分析[J]. 《中国康复理论与实践》, 2023, 29(5): 565-569. |
| [7] | 郭霜, 谢咏祺, 张良, 张春佳, 彭润, 杨德刚, 杨明亮. 舞蹈致儿童无骨折脱位型脊髓损伤神经学预后的影响因素及预测模型[J]. 《中国康复理论与实践》, 2023, 29(5): 582-589. |
| [8] | 高飞, 刘丽旭, 袁永学. 脑干卒中导致吞咽障碍的临床特征及康复[J]. 《中国康复理论与实践》, 2023, 29(4): 465-471. |
| [9] | 李经宇, 吕云, 辛雨, 李硕, 彭思静, 密忠祥. 城市医疗集团康复患者向下转诊意愿及影响因素[J]. 《中国康复理论与实践》, 2023, 29(12): 1481-1488. |
| [10] | 刘晓燕,丁霞,董晨,李荣,孙驰. 社区与住院老年人跌倒的现状及影响因素[J]. 《中国康复理论与实践》, 2022, 28(4): 389-398. |
| [11] | 葛章伟,黄馨,刘正东,张敏,张家奎. 重症监护室中老年患者术后谵妄影响因素分析及风险预测模型建立与评价[J]. 《中国康复理论与实践》, 2022, 28(3): 340-345. |
| [12] | 秦宁,沈志莹,石双姣,李旭红,钟竹青. 心脏康复转介服务[J]. 《中国康复理论与实践》, 2022, 28(3): 366-372. |
| [13] | 龚翔,潘颖颖,曾玲丽,杨清艳,周蕴弢,沈莹莹,范亚蓓,肖剑秋. 儿童康复治疗师的人格特质与职业满意度影响因素调查[J]. 《中国康复理论与实践》, 2022, 28(10): 1224-1230. |
| [14] | 蔡玮,邢文华,梁文平,赵雷,刘萍,滕珲,王国栋. 南皮县经皮冠状动脉介入治疗术后患者心脏康复现状调查[J]. 《中国康复理论与实践》, 2021, 27(8): 966-972. |
| [15] | 袁永学,张庆苏. 环咽肌功能障碍患者康复结局的影响因素[J]. 《中国康复理论与实践》, 2021, 27(8): 973-977. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
|
||