


《中国康复理论与实践》 ›› 2022, Vol. 28 ›› Issue (9): 1039-1048.doi: 10.3969/j.issn.1006-9771.2022.09.006
任开新1,李灵聪1,王秀静1,马力颖2,王振宇1( )
)
收稿日期:2021-12-22
修回日期:2022-04-15
出版日期:2022-09-25
发布日期:2022-10-08
通讯作者:
王振宇
E-mail:wangzhenyudr@163.com
作者简介:任开新(1993-),男,汉族,云南文山市人,硕士研究生,主要研究方向:骨科康复,疼痛康复。|王振宇(1980-),男,黑龙江哈尔滨市人,博士,主任医师,硕士生导师,主要研究方向:针灸推拿。
基金资助:
REN Kaixin1,LI Lingcong1,WANG Xiujing1,MA Liying2,WANG Zhenyu1()
Received:2021-12-22
Revised:2022-04-15
Published:2022-09-25
Online:2022-10-08
Contact:
WANG Zhenyu
E-mail:wangzhenyudr@163.com
Supported by:摘要:
目的 评估肩袖损伤的非手术治疗的总体治疗效应以及情景效应比例(PCE)。
方法 从PubMed、Embase、Cochrane Library、Web of Science、CINAHL、中国知网和万方数据库检索从建库至2020年10月关于肩袖损伤非手术治疗的随机对照试验(RCT)。由2名研究者独立进行文献筛选、资料提取和质量评价,采用STATA 15.0软件进行Meta分析。
结果 纳入40项研究,2 976例患者。疼痛总PCE为0.61 (95%CI 0.54~0.69)。各项治疗的PCE由大到小依次为皮质类固醇注射治疗、体外冲击波治疗、口服非甾体抗炎药、手法治疗、透明质酸注射治疗、富血小板血浆注射治疗、激光治疗、非甾体抗炎药注射治疗、针刺治疗。功能和活动范围的总PCE分别为0.69 (95%CI 0.61~0.77)和0.62 (95%CI 0.48~0.81)。盲法、在发达国家开展的研究、较长的治疗疗程均能增加疼痛的PCE。
结论 肩袖损伤非手术治疗效果中,61%与情景效应有关,较高的PCE可能是导致临床实践与临床研究结论不一致的原因。
中图分类号:
任开新,李灵聪,王秀静,马力颖,王振宇. 肩袖损伤非手术治疗效果中情景效应比例的Meta分析[J]. 《中国康复理论与实践》, 2022, 28(9): 1039-1048.
REN Kaixin,LI Lingcong,WANG Xiujing,MA Liying,WANG Zhenyu. Proportion of contextual effect of non-surgical treatments for rotator cuff injuries: a meta-analysis[J]. 《Chinese Journal of Rehabilitation Theory and Practice》, 2022, 28(9): 1039-1048.

图1
文献筛选流程图"
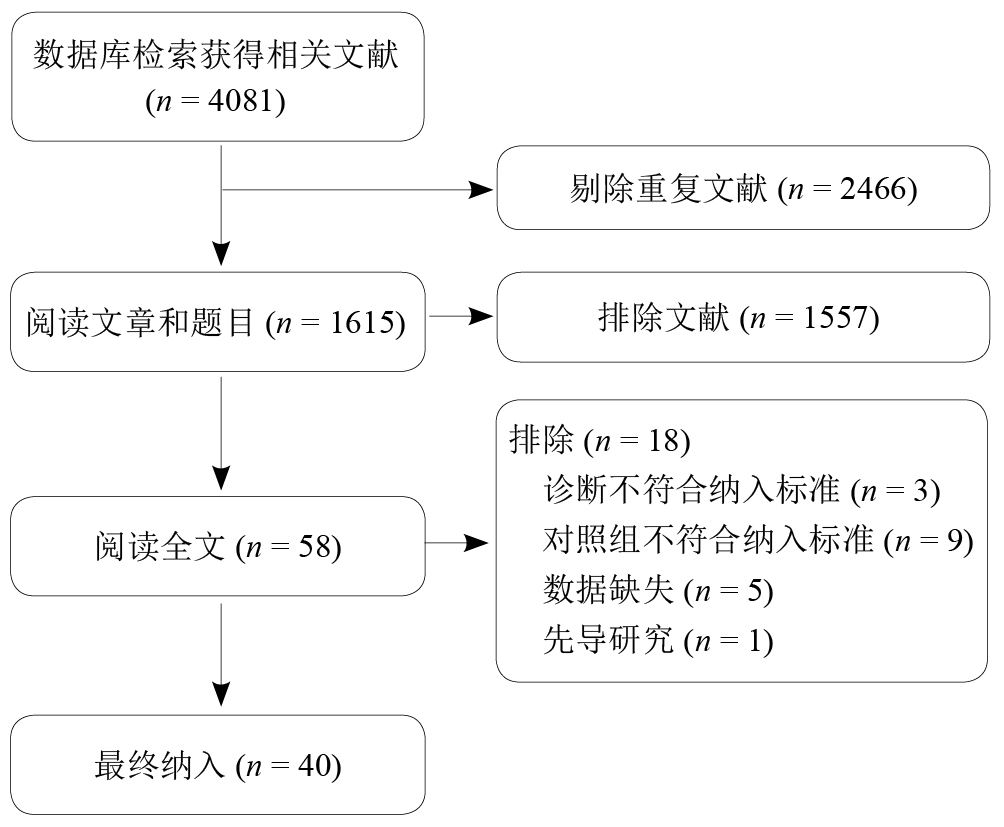
表1
纳入研究基本特征"
| 纳入研究 | 国家 | n | 年龄/岁 | 干预措施 | 治疗 次数 | 疗程 | 基础 治疗 | 止痛药物 | 结局指标 | 随访 时间 | Jadad 评分 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 试验组 | 对照组 | |||||||||||
| Alvarez-Nemegyei等[ | 墨西哥 | 56 | 52.5±8.9 | CS+利多卡因 | 利多卡因 | 1 | < 1周 | 理疗 | NSAIDs | VAS/SDQ/ ROM | 6个月 | 6 |
| Alvarez等[ | 加拿大 | 58 | 48.1±13.1 | CS+利多卡因 | 利多卡因 | 1 | < 1周 | 未提及 | 未提及 | VAS/DASH | 3个月 | 7 |
| Penning等[ | 荷兰 | 149 | 53.0±10.1 | HA+利多卡因;CS+利多卡因 | NS+利多卡因 | 3 | 6周 | 无 | 扑热息痛 | VAS/SDQ | 3~4.5个月 | 7 |
| Akgün等[ | 土耳其 | 32 | 48.5±8.5 | CS+利多卡因 | 利多卡因 | 2 | 20 d | 运动 | 萘普生 | VAS/CMS | 3个月 | 3 |
| Petri等[ | 美国 | 75 | 无数据 | CS+利多卡因+NSAIDs;利多卡因+NSAIDs | 利多卡+CS+安慰剂;利多卡因+安慰剂 | 1 | 30 d | 运动 | 扑热息痛 | VAS/临床指数/ROM | 1个月 | 6 |
| Hong等[ | 韩国 | 54 | 50.8±9.9 | CS+利多卡因 | 利多卡因 | 1 | < 1周 | 运动 | 禁止使用 | VAS/SDQ/ ROM | 8周 | 7 |
| Kesikburun等[ | 土耳其 | 40 | 48.5±11.4 | PRP+利多卡因 | NS+利多卡因 | 1 | < 1周 | 运动 | 扑热息痛 | VAS/SPADI | 12个月 | 7 |
| Schwitzguebel 等[ | 瑞士 | 80 | 47.9±13.9 | PRP | NS | 2 | 8周 | 无 | 扑热息痛 | VAS/CMS | 12个月 | 6 |
| Cai等[ | 中国 | 136 | 40.2±8.2 | PRP+利多卡因;HA+利多卡因 | NS+利多卡因 | 4 | 4周 | 未提及 | 未提及 | VAS/CMS | 6个月 | 5 |
| Rha等[ | 韩国 | 30 | 53.0±10.5 | PRP+利多卡因 | 干针刺+利多卡因 | 2 | 4周 | 运动 | 扑热息痛 | VAS/SPADI | 6个月 | 5 |
| Chou等[ | 中国 | 51 | 51.8±8.4 | HA | NS | 5 | 5周 | 无 | 未提及 | VAS/CMS | 1周 | 6 |
| Moghtaderi等[ | 伊朗 | 40 | 无数据 | HA | NS | 3 | 3周 | 未提及 | 未提及 | VAS/CMS | 3周 | 4 |
| Itzkowitch等[ | 英格兰 | 77 | 58.0±12.0 | NSAIDs注射 | 安慰剂注射 | 4 | 4周 | 未提及 | 扑热息痛 | VAS/临床指数/ROM | 4周 | 5 |
| Devereaux等[ | 加拿大 | 67 | 47.4±12.4 | NSAIDs+运动 | 运动 | 4 | 2周 | 运动 | 未提及 | VAS/CMS/ ROM | 2周 | 4 |
| Petri等[ | 美国 | 306 | 49.1±12.3 | 口服NSAIDs | 安慰剂 | 28 | 2周 | 未提及 | 未提及 | VAS/患者满意度/ROM | 2周 | 4 |
| Abrisham等[ | 伊朗 | 80 | 51.7±6.2 | 激光 | 假激光 | 10 | 2周 | 运动 | 无 | VAS/ROM | 2 周 | 4 |
| Yeldan等[ | 土耳其 | 60 | 55.2±8.7 | 激光 | 假激光 | 15 | 3周 | 运动 | 未提及 | VAS/SDQ/ ROM | 3 周 | 5 |
| Elsodany等[ | 埃及 | 60 | 50.2±3.7 | 激光 | 假激光 | 12 | 4周 | 运动 | 未提及 | VAS/SPADI/ROM | 0周 | 5 |
| Dogan等[ | 土耳其 | 52 | 53.6±11.3 | 激光 | 假激光 | 14 | 3周 | 运动 | 未提及 | VAS/SPADI/ROM | 0周 | 7 |
| Kibar等[ | 土耳其 | 62 | 60.0±10.0 | 激光 | 假激光 | 15 | 3周 | 运动 | 扑热息痛 | VAS/SPADI/ROM | 1 个月 | 5 |
| Vecchio等[ | 英格兰 | 35 | 52.0±16.3 | 激光 | 假激光 | 16 | 8周 | 运动 | 扑热息痛 | VAS/VAS/功能 | 2个月 | 4 |
| Kelle等[ | 土耳其 | 90 | 50.7±10.2 | 激光 | 假激光 | 9 | 3周 | 运动 | 扑热息痛 | VAS/UCLA肩关节评分 | 6个月 | 1 |
| Eslamian等[ | 伊朗 | 50 | 50.2±12.1 | 激光 | 无 | 10 | 3周 | 运动 | NSAIDs | VAS/SDQ/ROM | 3周 | 5 |
| Vas等[ | 西班牙 | 322 | 55.7±11.3 | 针刺 | 经皮神经电刺激 | 3 | 3周 | 运动 | NSAIDs/止痛药 | VAS/CMS | 12个月 | 7 |
| Lathia等[ | 美国 | 20 | 61.9±4.6 | 针刺 | 假针刺 | 12 | 6周 | 运动 | 未提及 | VAS/SPADI | 1.5个月 | 5 |
| Rueda等[ | 西班牙 | 68 | 33.4±12.5 | 针刺 | 假针刺 | 4 | 4周 | 未提及 | 未提及 | VAS/UCLA肩关节评分 | 0周 | 4 |
| Kvalvaag等[ | 挪威 | 130 | 46.8±10.2 | ESWT | 假ESWT | 4 | 4周 | 运动 | 未提及 | VAS/SPADI | 12个月 | 6 |
| Li等[ | 中国 | 84 | 47.7±9.9 | ESWT | 假ESWT | 5 | 15天 | 未提及 | 未提及 | VAS/CMS | 2个月 | 7 |
| Ko等[ | 中国 | 31 | 53.1±2.7 | ESWT | 假ESWT | 1 | < 1周 | 运动 | 扑热息痛 | VAS/CMS/ ROM | 12个月 | 6 |
| Kolk等[ | 荷兰 | 69 | 46.9±9.1 | ESWT | 假ESWT | 3 | 6周 | 无 | 止痛药 | VAS/CMS | 6个月 | 7 |
| Speed等[ | 英国 | 74 | 52.0±11.4 | ESWT | 假ESWT | 3 | 12周 | 无 | 无 | VAS/SPADI | 6个月 | 4 |
| Galasso等[ | 意大利 | 20 | 50.9±10.6 | ESWT | 假ESWT | 2 | 2周 | 未提及 | 扑热息痛 | VAS/CMS | 3个月 | 3 |
| Bennell等[ | 澳大利亚 | 120 | 59.3±10.1 | 手法治疗 | 假治疗 | 10 | 10周 | 无 | 止痛药 | VAS/SPADI | 22周 | 7 |
| Delgado-Gil等[ | 西班牙 | 42 | 55.0±9.0 | 手法治疗 | 假治疗 | 4 | 2周 | 无 | 禁止使用 | VAS/ROM | 1 d | 5 |
| Haik等[ | 西班牙 | 55 | 32.5±12.0 | 手法治疗 | 假治疗 | 2 | < 1周 | 未提及 | 未提及 | VAS/DASH | 2 d | 4 |
| Bertrand等[ | 加拿大 | 53 | 53.8±13.5 | 葡萄糖+利多卡因 | 利多卡因 | 3 | 3月 | 运动 | 对乙酰氨基酚 | VAS | 3个月 | 6 |
| Lin等[ | 中国 | 31 | 46.3±5.7 | 葡萄糖+利多卡因 | 利多卡因 | 1 | < 1周 | 未提及 | 未提及 | VAS/SPADI/ROM | 2周 | 6 |
| Yilmaz等[ | 土耳其 | 28 | 51.6±9.7 | SWD | 假SWD | 10 | 2周 | 运动 冷敷 | 美洛昔康 | VAS/SDQ/ ROM | 2个月 | 7 |
| Galace de Freitas等[ | 巴西 | 46 | 50.5±8.9 | PEMF | 假PEMF | 9 | 3周 | 运动 | 未提及 | VAS/CMS | 1 d | 6 |
| Aceituno-Gómez等[ | 西班牙 | 43 | 59.1±9.1 | 激光 | 假激光 | 15 | 3周 | 运动 | 止痛药 | VAS/SPADI/ROM | 3个月 | 2 |

图2
独立文献偏倚风险评估图 注:+,符合;—,不符合;?,不确定。"

表2
肩袖损伤非手术治疗措施的治疗效应与PCE"
| 结局指标 | 治疗措施 | 研究数量 | 样本量 | 治疗效应 (95% CI) | I2/% | PCE (95% CI) | I2/% |
|---|---|---|---|---|---|---|---|
| 疼痛 | 皮质类固醇注射 | 6 | 314 | 1.12 (0.77~1.62) | 58.4 | 0.79 (0.56~1.10) | 46.1 |
| 富血小板血浆注射 | 4 | 219 | 2.05 (1.31~3.21) | 42.9 | 0.60 (0.39~0.91) | 78.6 | |
| 透明质酸注射 | 4 | 231 | 1.47 (0.70~3.11) | 85.0 | 0.62 (0.37~1.03) | 75.0 | |
| 增生疗法 | 2 | 84 | 2.53 (0.56~11.5) | 76.3 | 0.62 (0.41~0.95) | 3.5 | |
| NSAIDs 注射 | 1 | 77 | 2.18 (1.23~3.85) | - | 0.36 (0.23~0.55) | - | |
| NSAIDs口服 | 3 | 410 | 1.10 (0.91~1.33) | 0 | 0.76 (0.60~0.95) | 0 | |
| 激光治疗 | 9 | 532 | 1.93 (1.40~2.66) | 49.3 | 0.54 (0.42~0.69) | 82.3 | |
| 针刺治疗 | 3 | 410 | 1.66 (1.32~2.09) | 0 | 0.36 (0.28~0.46) | 0 | |
| 体外冲击波治疗 | 6 | 408 | 1.24 (0.83~1.87) | 67.1 | 0.76 (0.51~1.13) | 78.0 | |
| 手法 | 3 | 217 | 0.59 (0.34~1.02) | 72.1 | 0.72 (0.47~1.12) | 0 | |
| 其他 | 2 | 74 | 1.71 (0.74~3.97) | 46.2 | 0.41 (0.10~1.73) | 85.6 | |
| 合计 | 43 | 2976 | 1.41 (1.20~1.65) | 69.9 | 0.61 (0.54~0.69) | 78.1 | |
| 功能 | 皮质类固醇注射 | 6 | 314 | 1.13 (0.81~1.56) | 49.1 | 0.83 (0.60~1.14) | 37.0 |
| 富血小板血浆注射 | 4 | 219 | 2.14 (0.75~6.16) | 86.2 | 0.54 (0.29~1.00) | 75.0 | |
| 透明质酸注射 | 4 | 231 | 1.29 (0.47~3.54) | 90.8 | 0.47 (0.17~1.30) | 82.0 | |
| 增生疗法 | 1 | 31 | 0.85 (0.41~1.76) | - | 0.33 (0.05~2.20) | - | |
| NSAIDs 注射 | 1 | 77 | 1.67 (0.99~2.81) | - | 0.46 (0.30~0.73) | - | |
| NSAIDs口服 | 3 | 410 | 1.75 (0.92~3.32) | 73.5 | 0.71 (0.60~0.84) | 41.1 | |
| 激光治疗 | 8 | 452 | 1.39 (1.06~1.83) | 31.0 | 0.73 (0.53~0.99) | 77.6 | |
| 针刺治疗 | 3 | 472 | 1.83 (1.47~2.27) | 0 | 0.53 (0.46~0.62) | 0 | |
| 体外冲击波治疗 | 6 | 408 | 1.18 (0.90~1.55) | 28.9 | 0.79 (0.65~0.97) | 35.4 | |
| 手法 | 2 | 175 | 1.75 (0.54~5.66) | 84.6 | 0.27 (0.02~3.48) | 87.7 | |
| 其他 | 2 | 75 | 1.10 (0.67~1.81) | 0 | 0.63 (0.26~1.51) | 41.6 | |
| 合计 | 40 | 2864 | 1.37 (1.17~1.62) | 69.7 | 0.69 (0.61~0.77) | 71.9 | |
| ROM | 合计 | 16 | 1034 | 1.02 (0.72~1.43) | 81.6 | 0.62 (0.48~0.81) | 84.0 |

图3
疼痛的治疗效应和PCE等级排序图"
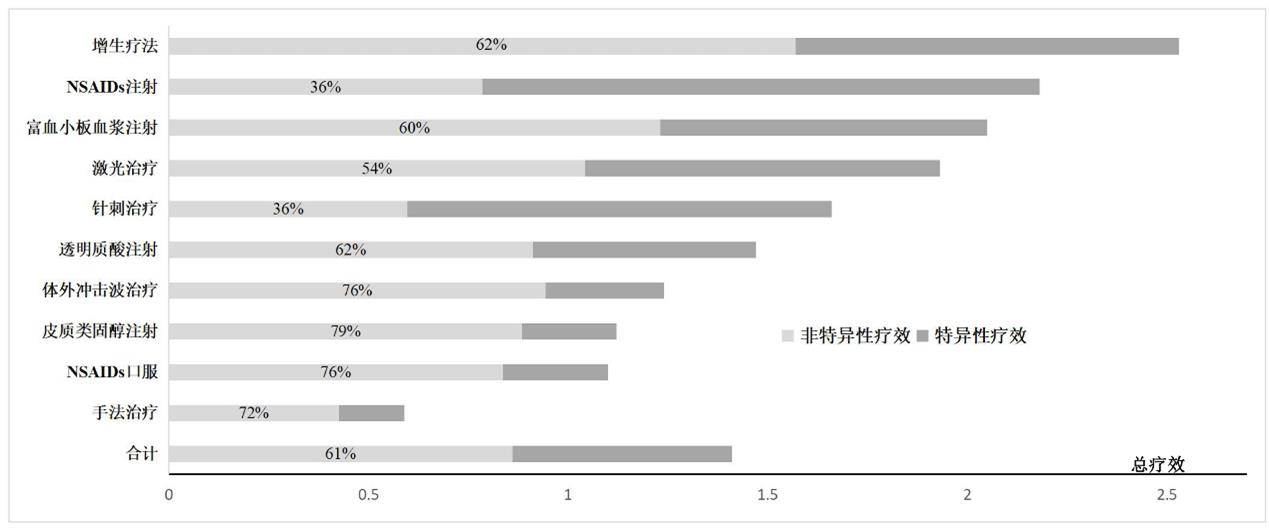
表3
疼痛亚组分析结果"
| 亚组 | 研究数量 | n | 治疗效应 (95% CI) | I2/% | PCE (95% CI) | I2/% | |
|---|---|---|---|---|---|---|---|
| 疗程 | ≤ 4周 | 30 | 2196 | 1.53 (1.25~1.88) | 73.9 | 0.57 (0.48~0.67) | 82.5 |
| > 4周 | 13 | 780 | 1.16 (0.94~1.44) | 47.6 | 0.73 (0.61~0.86) | 32.9 | |
| 参与者年龄 | < 40岁 | 3 | 190 | 1.38 (0.59~3.22) | 85.7 | 0.40 (0.26~0.63) | 25.4 |
| 40~50岁 | 11 | 966 | 1.20 (0.91~1.58) | 69.9 | 0.75 (0.59~0.97) | 71.9 | |
| 50~60岁 | 27 | 1738 | 1.47 (1.20~1.82) | 68.6 | 0.61 (0.53~0.70) | 74.6 | |
| ≥ 60岁 | 2 | 82 | 2.71 (1.44~5.10) | 0 | 0.15 (0.07~0.33) | 0 | |
| 损伤类型 | 肩袖肌腱炎 | 18 | 1585 | 1.38 (1.10~1.74) | 70.0 | 0.57 (0.48~0.67) | 76.9 |
| 肩峰撞击综合征 | 16 | 940 | 1.21 (0.91~1.60) | 73.5 | 0.71 (0.55~0.91) | 75.4 | |
| 肩袖肌腱撕裂 | 7 | 377 | 1.98 (1.50~2.63) | 22.6 | 0.57 (0.42~0.77) | 75.1 | |
| 给药途径 | 注射治疗 | 17 | 925 | 1.54 (1.16~2.05) | 71.6 | 0.64 (0.53~0.77) | 67.5 |
| 口服药物 | 3 | 410 | 1.10 (0.91~1.33) | 0 | 0.76 (0.60~0.95) | 0 | |
| 物理治疗 | 23 | 1641 | 1.42 (1.13~1.80) | 72.4 | 0.56 (0.46~0.69) | 82.9 | |
| 是否充分隐藏 | 是 | 24 | 1665 | 1.36 (1.07~1.73) | 75.8 | 0.64 (0.52~0.78) | 84.7 |
| 否 | 19 | 1311 | 1.49 (1.22~1.82) | 56.9 | 0.58 (0.50~0.67) | 56.1 | |
| 患者是否盲法 | 是 | 32 | 2117 | 1.34 (1.10~1.62) | 73.1 | 0.65 (0.57~0.75) | 71.5 |
| 否 | 11 | 859 | 1.68 (1.26~2.22) | 55.6 | 0.52 (0.41~0.67) | 77.2 | |
| 国家经济水平 | 发展中国家 | 19 | 1029 | 1.89 (1.44~2.47) | 65.1 | 0.55 (0.46~0.67) | 80.4 |
| 发达国家 | 24 | 1947 | 1.16 (0.96~1.39) | 67.6 | 0.66 (0.55~0.79) | 73.1 | |
| 资金来源 | 公共 | 16 | 1142 | 1.49 (1.16~1.90) | 64.8 | 0.54 (0.44~0.67) | 70.6 |
| 企业 | 4 | 523 | 1.13 (0.95~1.34) | 0 | 0.86 (0.53~1.39) | 82.0 | |
| 是否联合治疗 | 是 | 31 | 2031 | 1.53 (1.29~1.82) | 59.5 | 0.63 (0.54~0.73) | 81.9 |
| 否 | 12 | 945 | 1.13 (0.81~1.59) | 81.3 | 0.55 (0.42~0.72) | 56.7 | |
| 随访时间 | 治疗后即刻 | 3 | 180 | 2.37 (1.40~4.00) | 27.5 | 0.51 (0.39~0.68) | 68.7 |
| ≤ 3个月 | 26 | 1545 | 1.32 (1.06~1.65) | 71.1 | 0.61 (0.53~0.70) | 50.1 | |
| 3~6个月 | 8 | 575 | 1.54 (1.14~2.09) | 60.4 | 0.62 (0.45~0.87) | 78.6 | |
| > 6个月 | 6 | 676 | 1.32 (0.90~1.94) | 75.8 | 0.72 (0.44~1.17) | 91.1 | |
表4
功能亚组分析结果"
| 亚组 | 研究数量 | n | 治疗效应(95% CI) | I2/% | PCE(95% CI) | I2/% | |
|---|---|---|---|---|---|---|---|
| 疗程 | ≤ 4周 | 11 | 673 | 1.55(1.30~1.84) | 58.9 | 0.66(0.58~0.76) | 77.8 |
| > 4周 | 29 | 2191 | 0.99(0.74~1.31) | 65.8 | 0.69(0.61~0.79) | 0 | |
| 参与者年龄 | < 40岁 | 3 | 190 | 2.97(1.79~4.93) | 30.7 | 0.13(0.03~0.63) | 79.5 |
| 40~50岁 | 11 | 966 | 1.16(0.85~1.58) | 76.1 | 0.80(0.64~1.00) | 52.3 | |
| 50~60岁 | 24 | 1626 | 1.33(1.08~1.63) | 64.9 | 0.71(0.62~0.80) | 70.3 | |
| ≥ 60岁 | 2 | 82 | 2.13(1.21~3.76) | 0 | 0.24(0.08~0.78) | 59.6 | |
| 损伤类型 | 肩袖肌腱炎 | 16 | 1514 | 1.35(1.09~1.69) | 63.5 | 0.68(0.60~0.78) | 72.4 |
| 肩峰撞击综合征 | 15 | 899 | 1.25(0.96~1.61) | 67.3 | 0.76(0.59~0.98) | 69.1 | |
| 肩袖肌腱撕裂 | 7 | 377 | 2.00(1.01~3.98) | 83.8 | 0.45(0.27~0.77) | 77.7 | |
| 治疗途径 | 注射治疗 | 16 | 872 | 1.33(0.95~1.85) | 79.0 | 0.61(0.46~0.82) | 68.1 |
| 口服药物 | 3 | 410 | 1.75(0.92~3.32) | 73.5 | 0.71(0.60~0.84) | 41.1 | |
| 物理治疗 | 21 | 1582 | 1.38(1.17~1.63) | 42.4 | 0.70(0.60~0.82) | 75.5 | |
| 是否充分隐藏 | 是 | 22 | 1606 | 1.17(0.94~1.46) | 69.6 | 0.77(0.68~0.89) | 66.2 |
| 否 | 18 | 1258 | 1.66(1.31~2.09) | 62.7 | 0.56(0.45~0.70) | 71.1 | |
| 是否盲法 | 是 | 29 | 2005 | 1.31(1.07~1.61) | 73.9 | 0.72(0.62~0.84) | 66.0 |
| 否 | 11 | 859 | 1.65(1.41~1.93) | 0 | 0.60(0.48~0.74) | 76.4 | |
| 国家经济水平 | 发展中国家 | 18 | 950 | 1.59(1.22~2.07) | 60.9 | 0.65(0.53~0.79) | 75.8 |
| 发达国家 | 22 | 1914 | 1.25(1.01~1.55) | 74.8 | 0.70(0.60~0.81) | 59.8 | |
| 基金来源 | 公共 | 15 | 1151 | 1.64(1.23~2.20) | 69.5 | 0.66(0.54~0.81) | 72.0 |
| 企业 | 4 | 523 | 1.33(0.91~1.93) | 64.3 | 0.83(0.65~1.07) | 40.1 | |
| 是否联合治疗 | 是 | 29 | 1961 | 1.30(1.09~1.56) | 62.9 | 0.72(0.64~0.81) | 68.8 |
| 否 | 11 | 903 | 1.57(1.07~2.30) | 80.0 | 0.51(0.34~0.75) | 77.6 | |
| 随访时间 | 治疗后即刻 | 3 | 180 | 1.52(0.64~3.61) | 67.5 | 0.80(0.47~1.36) | 87.2 |
| ≤ 3个月 | 23 | 1371 | 1.29(1.07~1.56) | 53.7 | 0.66(0.56~0.79) | 53.6 | |
| 3~6个月 | 8 | 575 | 1.88(1.28~2.77) | 68.3 | 0.58(0.4~0.85) | 79.4 | |
| > 6个月 | 6 | 738 | 1.17(0.67~2.07) | 89.5 | 0.71(0.55~0.93) | 72.1 | |
| [1] |
WALACH H. The efficacy paradox in randomized controlled trials of CAM and elsewhere: beware of the placebo trap[J]. J Altern Complem Med, 2001, 7(3): 213-218.
pmid: 11439833 |
| [2] |
ZOU K, WONG J, ABDULLAH N, et al. Examination of overall treatment effect and the proportion attributable to contextual effect in osteoarthritis: meta-analysis of randomised controlled trials[J]. Ann Rheum Dis, 2016, 75(11): 1964-1970.
doi: 10.1136/annrheumdis-2015-208387 pmid: 26882927 |
| [3] |
DI BLASI Z, HARKNESS E, ERNST E, et al. Influence of context effects on health outcomes: a systematic review[J]. Lancet, 2001, 357(9258): 757-762.
pmid: 11253970 |
| [4] |
ROSSETTINI G, CARLINO E, TESTA M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain[J]. BMC Musculoskelet Disord, 2018, 19(1): 27.
doi: 10.1186/s12891-018-1943-8 |
| [5] |
LUIME J J, KOES B W, HENDRIKSEN I J, et al. Prevalence and incidence of shoulder pain in the general population; a systematic review[J]. Scand J Rheumatol, 2004, 33(2): 73-81.
pmid: 15163107 |
| [6] |
TEKAVEC E, JÖUD A, RITTNER R, et al. Population-based consultation patterns in patients with shoulder pain diagnoses[J]. BMC Musculoskelet Disord, 2012, 13: 238.
doi: 10.1186/1471-2474-13-238 |
| [7] |
WEBER S, CHAHAL J. Management of rotator cuff injuries[J]. J Am Acad Orthop Surg, 2020, 28(5): e193-e201.
doi: 10.5435/JAAOS-D-19-00463 |
| [8] | 张凯搏, 唐新, 李箭, 等. 2019年美国骨科医师学会(AAOS)肩袖损伤临床实践指南解读[J]. 中国运动医学杂志, 2020, 39(5): 403-412. |
| ZHANG K B, TANG X, LI J, et al. Interpretation of the 2019 American Academy of Orthopaedic Surgeons (AAOS) Management of Rotator Cuff Injuries Clinical Practice Guideline[J]. Chin J Sports Med, 2020, 39(5):403-412. | |
| [9] |
BOUDREAULT J, DESMEULES F, ROY J S, et al. The efficacy of oral non-steroidal anti-inflammatory drugs for rotator cuff tendinopathy: a systematic review and meta-analysis[J]. J Rehabil Med, 2014, 46(4): 294-306.
doi: 10.2340/16501977-1800 pmid: 24626286 |
| [10] |
CHEN X, JONES I A, TOGASHI R, et al. Use of platelet-rich plasma for the improvement of pain and function in rotator cuff tears: a systematic review and meta-analysis with bias assessment[J]. Am J Sports Med, 2020, 48(8): 2028-2041.
doi: 10.1177/0363546519881423 pmid: 31743037 |
| [11] |
LIN M T, CHIANG C F, WU C H, et al. Comparative effectiveness of injection therapies in rotator cuff tendinopathy: a systematic review, pairwise and network meta-analysis of randomized controlled trials[J]. Arch Phys Med Rehabil, 2019, 100(2): 336-349.e15.
doi: 10.1016/j.apmr.2018.06.028 |
| [12] |
MOHAMADI A, CHAN J J, CLAESSEN F M, et al. Corticosteroid injections give small and transient pain relief in rotator cuff tendinosis: a meta-analysis[J]. Clin Orthop Relat Res, 2017, 475(1): 232-243.
doi: 10.1007/s11999-016-5002-1 |
| [13] | PAGE M J, GREEN S, MROCKI M A, et al. Electrotherapy modalities for rotator cuff disease[J]. Cochrane Database Syst Rev (Online), 2016, 2016(6): CD012225. |
| [14] |
MOHER D, LIBERATI A, TETZLAFF J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement[J]. BMJ, 2009, 339: b2535.
doi: 10.1136/bmj.b2535 |
| [15] |
ANGST F, SCHWYZER H K, AESCHLIMANN A, et al. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and its short version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form, Constant (Murley) Score (CS), Simple Shoulder Test (SST), Oxford Shoulder Score (OSS), Shoulder Disability Questionnaire (SDQ), and Western Ontario Shoulder Instability Index (WOSI)[J]. Arthritis Care Res (Hoboken), 2011, 63(Suppl 11): S174-S188.
doi: 10.1002/acr.20630 |
| [16] | HIGGINS J P T, THOMAS J, CHANDLER J, et al. Cochrane Handbook for Systematic Reviews of Interventions[M]. 2nd ed. Chichester, UK: John Wiley & Sons, 2019. |
| [17] |
CLARK H D, WELLS G A, HUËT C, et al. Assessing the quality of randomized trials: reliability of the Jadad scale[J]. Control Clin Trials, 1999, 20(5): 448-452.
doi: 10.1016/s0197-2456(99)00026-4 pmid: 10503804 |
| [18] | HEDGES L V, OLKIN I. Statistical Methods for Meta-Analysis[M]. San Diego, CA: Academic Press, 1985. |
| [19] |
ALVAREZ-NEMEGYEI J, BASSOL-PEREA A, ROSADO PASOS J. Efficacy of the local injection of methylprednisolone acetate in the subacromial impingement syndrome. a randomized, double-blind trial[J]. Reumatol Clin, 2008, 4(2): 49-54.
doi: 10.1016/S1699-258X(08)71799-6 |
| [20] |
ALVAREZ C M, LITCHFIELD R, JACKOWSKI D, et al. A prospective, double-blind, randomized clinical trial comparing subacromial injection of betamethasone and xylocaine to xylocaine alone in chronic rotator cuff tendinosis[J]. Am J Sports Med, 2005, 33(2): 255-262.
doi: 10.1177/0363546504267345 |
| [21] | PENNING L I, DE BIE R A, WALENKAMP G H. The effectiveness of injections of hyaluronic acid or corticosteroid in patients with subacromial impingement: a three-arm randomised controlled trial[J]. J Bone Joint Surg Br, 2012, 94(9): 1246-1252. |
| [22] |
AKGÜN K, BIRTANE M, AKARIRMAK U. Is local subacromial corticosteroid injection beneficial in subacromial impingement syndrome?[J]. Clin Rheumatol, 2004, 23(6): 496-500.
pmid: 15278758 |
| [23] |
PETRI M, DOBROW R, NEIMAN R, et al. Randomized, double-blind, placebo-controlled study of the treatment of the painful shoulder[J]. Arthritis Rheum, 1987, 30(9): 1040-1045.
doi: 10.1002/art.1780300911 |
| [24] |
HONG J Y, YOON S H, MOON D J, et al. Comparison of high- and low-dose corticosteroid in subacromial injection for periarticular shoulder disorder: a randomized, triple-blind, placebo-controlled trial[J]. Arch Phys Med Rehabil, 2011, 92(12): 1951-1960.
doi: 10.1016/j.apmr.2011.06.033 |
| [25] |
KESIKBURUN S, TAN A K, YILMAZ B, et al. Platelet-rich plasma injections in the treatment of chronic rotator cuff tendinopathy: a randomized controlled trial with 1-year follow-up[J]. Am J Sports Med, 2013, 41(11): 2609-2616.
doi: 10.1177/0363546513496542 pmid: 23893418 |
| [26] |
SCHWITZGUEBEL A J, KOLO F C, TIREFORT J, et al. Efficacy of platelet-rich plasma for the treatment of interstitial supraspinatus tears: a double-blinded, randomized controlled trial[J]. Am J Sports Med, 2019, 47(8): 1885-1892.
doi: 10.1177/0363546519851097 pmid: 31161947 |
| [27] | CAI Y U, SUN Z, LIAO B, et al. Sodium hyaluronate and platelet-rich plasma for partial-thickness rotator cuff tears[J]. Med Sci Sports Exerc, 2019, 51(2): 227-233. |
| [28] |
RHA D W, PARK G Y, KIM Y K, et al. Comparison of the therapeutic effects of ultrasound-guided platelet-rich plasma injection and dry needling in rotator cuff disease: a randomized controlled trial[J]. Clin Rehabil, 2013, 27(2): 113-122.
doi: 10.1177/0269215512448388 |
| [29] |
CHOU W Y, KO J Y, WANG F S, et al. Effect of sodium hyaluronate treatment on rotator cuff lesions without complete tears: a randomized, double-blind, placebo-controlled study[J]. J Shoulder Elbow Surg, 2010, 19(4): 557-563.
doi: 10.1016/j.jse.2009.08.006 |
| [30] |
MOGHTADERI A, SAJADIYEH S, KHOSRAWI S, et al. Effect of subacromial sodium hyaluronate injection on rotator cuff disease: a double-blind placebo-controlled clinical trial[J]. Adv Biomed Res, 2013, 2: 89.
doi: 10.4103/2277-9175.122517 pmid: 24524035 |
| [31] |
ITZKOWITCH D, GINSBERG F, LEON M, et al. Peri-articular injection of tenoxicam for painful shoulders: a double-blind, placebo controlled trial[J]. Clin Rheumatol, 1996, 15(6): 604-609.
pmid: 8973872 |
| [32] |
DEVEREAUX M, VELANOSKI K Q, PENNINGS A, et al. Short-term effectiveness of precut kinesiology tape versus an NSAID as adjuvant treatment to exercise for subacromial impingement: a randomized controlled trial[J]. Clin J Sport Med, 2016, 26(1): 24-32.
doi: 10.1097/JSM.0000000000000187 pmid: 25915145 |
| [33] |
PETRI M, HUFMAN S L, WASER G, et al. Celecoxib effectively treats patients with acute shoulder tendinitis/bursitis[J]. J Rheumatol, 2004, 31(8): 1614-1620.
pmid: 15290743 |
| [34] |
ABRISHAM S M, KERMANI-ALGHORAISHI M, GHAHRAMANI R, et al. Additive effects of low-level laser therapy with exercise on subacromial syndrome: a randomised, double-blind, controlled trial[J]. Clin Rheumatol, 2011, 30(10): 1341-1346.
doi: 10.1007/s10067-011-1757-7 pmid: 21538218 |
| [35] |
YELDAN I, CETIN E, OZDINCLER A R. The effectiveness of low-level laser therapy on shoulder function in subacromial impingement syndrome[J]. Disabil Rehabil, 2009, 31(11): 935-940.
doi: 10.1080/09638280802377985 pmid: 19031167 |
| [36] |
ELSODANY A M, ALAYAT M, ALI M, et al. Long-term effect of pulsed Nd:YAG laser in the treatment of patients with rotator cuff tendinopathy: a randomized controlled trial[J]. Photomed Laser Surg, 2018, 36(9): 506-513.
doi: 10.1089/pho.2018.4476 pmid: 30188253 |
| [37] |
DOGAN S K, AY S, EVCIK D. The effectiveness of low laser therapy in subacromial impingement syndrome: a randomized placebo controlled double-blind prospective study[J]. Clinics (Sao Paulo), 2010, 65(10): 1019-1022.
doi: S1807-59322010001000016 pmid: 21120304 |
| [38] |
KIBAR S, KONAK H E, EVCIK D, et al. Laser acupuncture treatment improves pain and functional status in patients with subacromial impingement syndrome: a randomized, double-blind, sham-controlled study[J]. Pain Med, 2017, 18(5): 980-987.
doi: 10.1093/pm/pnw197 pmid: 27816913 |
| [39] |
VECCHIO P C, HAZLEMAN B L, KING R H. A double-blind trial comparing subacromial methylprednisolone and lignocaine in acute rotator cuff tendinitis[J]. Br J Rheumatol, 1993, 32(8): 743-745.
pmid: 8348279 |
| [40] |
KELLE B, KOZANOGLU E. Low-level laser and local corticosteroid injection in the treatment of subacromial impingement syndrome: a controlled clinical trial[J]. Clin Rehabil, 2014, 28(8): 762-771.
pmid: 24519921 |
| [41] |
ESLAMIAN F, SHAKOURI S K, GHOJAZADEH M, et al. Effects of low-level laser therapy in combination with physiotherapy in the management of rotator cuff tendinitis[J]. Lasers Med Sci, 2012, 27(5): 951-958.
doi: 10.1007/s10103-011-1001-3 |
| [42] |
VAS J, ORTEGA C, OLMO V, et al. Single-point acupuncture and physiotherapy for the treatment of painful shoulder: a multicentre randomized controlled trial[J]. Rheumatology (Oxford), 2008, 47(6): 887-893.
doi: 10.1093/rheumatology/ken040 pmid: 18403402 |
| [43] |
LATHIA A T, JUNG S M, CHEN L X. Efficacy of acupuncture as a treatment for chronic shoulder pain[J]. J Altern Complement Med, 2009, 15(6): 613-618.
doi: 10.1089/acm.2008.0272 |
| [44] |
RUEDA GARRIDO J C, VAS J, LOPEZ D R. Acupuncture treatment of shoulder impingement syndrome: a randomized controlled trial[J]. Complement Ther Med, 2016, 25: 92-97.
doi: 10.1016/j.ctim.2016.01.003 pmid: 27062955 |
| [45] | KVALVAAG E, ROE C, ENGEBRETSEN K B, et al. One year results of a randomized controlled trial on radial extracorporeal shock wave treatment, with predictors of pain, disability and return to work in patients with subacromial pain syndrome[J]. Eur J Phys Rehabil Med, 2018, 54(3): 341-350. |
| [46] |
LI W, ZHANG S X, YANG Q, et al. Effect of extracorporeal shock-wave therapy for treating patients with chronic rotator cuff tendonitis[J]. Medicine (Baltimore), 2017, 96(35): e7940.
doi: 10.1097/MD.0000000000007940 |
| [47] | KO J Y, SIU K K, WANG F S, et al. The Therapeutic effects of extracorporeal shock wave therapy (ESWT) on the rotator cuff lesions with shoulder stiffness: a prospective randomized study[J]. Biomed Res Int, 2020, 2020: 6501714. |
| [48] |
KOLK A, YANG K G, TAMMINGA R, et al. Radial extracorporeal shock-wave therapy in patients with chronic rotator cuff tendinitis: a prospective randomised double-blind placebo-controlled multicentre trial[J]. Bone Joint J, 2013, 95-B(11): 1521-1526.
doi: 10.1302/0301-620X.95B11.31879 pmid: 24151273 |
| [49] |
SPEED C A, RICHARDS C, NICHOLS D, et al. Extracorporeal shock-wave therapy for tendonitis of the rotator cuff: a double-blind, randomised, controlled trial[J]. J Bone Joint Surg Br, 2002, 84(4): 509-512.
doi: 10.1302/0301-620X.84B4.0840509 |
| [50] |
GALASSO O, AMELIO E, RICCELLI D A, et al. Short-term outcomes of extracorporeal shock wave therapy for the treatment of chronic non-calcific tendinopathy of the supraspinatus: a double-blind, randomized, placebo-controlled trial[J]. BMC Musculoskelet Disord, 2012, 13: 86.
doi: 10.1186/1471-2474-13-86 |
| [51] |
BENNELL K, WEE E, COBURN S, et al. Efficacy of standardised manual therapy and home exercise programme for chronic rotator cuff disease: randomised placebo controlled trial[J]. BMJ, 2010, 340: c2756.
doi: 10.1136/bmj.c2756 |
| [52] |
DELGADO-GIL J A, PRADO-ROBLES E, RODRIGUES-DE-SOUZA D P, et al. Effects of mobilization with movement on pain and range of motion in patients with unilateral shoulder impingement syndrome: a randomized controlled trial[J]. J Manipulative Physiol Ther, 2015, 38(4): 245-252.
doi: 10.1016/j.jmpt.2014.12.008 |
| [53] |
HAIK M N, ALBURQUERQUE-SENDíN F, CAMARGO P R. Short-term effects of thoracic spine manipulation on shoulder impingement syndrome: a randomized controlled trial[J]. Arch Phys Med Rehabil, 2017, 98(8): 1594-1605.
doi: 10.1016/j.apmr.2017.02.003 |
| [54] |
BERTRAND H, REEVES K D, BENNETT C J, et al. Dextrose prolotherapy versus control injections in painful rotator cuff tendinopathy[J]. Arch Phys Med Rehabil, 2016, 97(1): 17-25.
doi: 10.1016/j.apmr.2015.08.412 |
| [55] | LIN C L, HUANG C C, HUANG S W. Effects of hypertonic dextrose injection in chronic supraspinatus tendinopathy of the shoulder: a randomized placebo-controlled trial[J]. Eur J Phys Rehabil Med, 2019, 55(4): 480-487. |
| [56] |
YILMAZ KAYSIN M, AKPINAR P, AKTAS I, et al. Effectiveness of shortwave diathermy for subacromial impingement syndrome and value of night pain for patient selection: a double-blinded, randomized, placebo-controlled trial[J]. Am J Phys Med Rehabil, 2018, 97(3): 178-186.
doi: 10.1097/PHM.0000000000000819 |
| [57] |
GALACE DE FREITAS D, MARCONDES F B, MONTEIRO R L, et al. Pulsed electromagnetic field and exercises in patients with shoulder impingement syndrome: a randomized, double-blind, placebo-controlled clinical trial[J]. Arch Phys Med Rehabil, 2014, 95(2): 345-352.
doi: 10.1016/j.apmr.2013.09.022 |
| [58] |
ACEITUNO-GÓMEZ J, AVENDAÑO-COY J, GÓMEZ-SORIANO J, et al. Efficacy of high-intensity laser therapy in subacromial impingement syndrome: a three-month follow-up controlled clinical trial[J]. Clin Rehabil, 2019, 33(5): 894-903.
doi: 10.1177/0269215518824691 |
| [59] |
CHEN A T, SHRESTHA S, COLLINS J E, et al. Estimating contextual effect in nonpharmacological therapies for pain in knee osteoarthritis: a systematic analytic review[J]. Osteoarthr Cartilage, 2020, 28(9): 1154-1169.
doi: S1063-4584(20)31019-0 pmid: 32416220 |
| [60] |
WHITESIDE N, SARMANOVA A, CHEN X, et al. Proportion of contextual effects in the treatment of fibromyalgia: a meta-analysis of randomised controlled trials[J]. Clin Rheumatol, 2018, 37(5): 1375-1382.
doi: 10.1007/s10067-017-3948-3 |
| [61] |
BENEDETTI F. Placebo analgesia[J]. Neurol Sci, 2006, 27(Suppl 2): S100-S102.
doi: 10.1007/s10072-006-0580-4 |
| [62] |
COLLOCA L. The placebo effect in pain therapies[J]. Annu Rev Pharmacol Toxicol, 2019, 59: 191-211.
doi: 10.1146/annurev-pharmtox-010818-021542 pmid: 30216744 |
| [63] |
BERTHELOT J M, NIZARD J, MAUGARS Y. The negative Hawthorne effect: explaining pain overexpression[J]. Joint Bone Spine, 2019, 86(4): 445-449.
doi: 10.1016/j.jbspin.2018.10.003 |
| [64] |
ALRUTHIA Y, ALGHADEER S, BALKHI B, et al. Efficacy of acetaminophen versus ibuprofen for the management of rotator cuff-related shoulder pain: randomized open-label study[J]. Saudi Pharm J, 2019, 27(6): 882-888.
doi: 10.1016/j.jsps.2019.06.001 |
| [1] | 王贺, 韩靓, 阚梦凡, 于少泓. 电刺激治疗脑卒中后肩手综合征有效性的系统评价与Meta分析[J]. 《中国康复理论与实践》, 2023, 29(9): 1048-1056. |
| [2] | 于歌, 王璐, 陈亚平. 全身振动训练对慢性踝关节不稳姿势稳定性影响的Meta分析[J]. 《中国康复理论与实践》, 2023, 29(4): 423-432. |
| [3] | 张丽英, 王杰宁, 于小明. 机器人辅助训练对脑卒中患者上肢运动功能效果的Meta分析[J]. 《中国康复理论与实践》, 2023, 29(2): 156-166. |
| [4] | 孙喜妹, 刘华, 柴良伟, 李凯洋, 马景. 治疗性运动对头前倾并发颈痛患者颈部功能和生活质量影响的Meta分析[J]. 《中国康复理论与实践》, 2023, 29(2): 214-222. |
| [5] | 彭娟,王洁萍,黄炜,樊必双,虞记华,曾今,黄丽衡,安丽娟,胥方元. 阈值负荷吸气肌训练对慢性阻塞性肺疾病患者呼吸功能、运动功能及生活质量影响的Meta分析[J]. 《中国康复理论与实践》, 2022, 28(9): 1022-1031. |
| [6] | 徐振,王一迪,张月,温宇红. 运动干预对多发性硬化患者疲劳症状影响的Meta分析[J]. 《中国康复理论与实践》, 2022, 28(5): 568-577. |
| [7] | 曾晓霞,林荣,杨芳洁,肖鸿伟,苏雁,黄承武,何坚. 温针灸治疗肩袖损伤的效果[J]. 《中国康复理论与实践》, 2022, 28(5): 609-615. |
| [8] | 郑尉,孙立冰,郝传萍,黄文琪,尤婧,郭彦桦. 脊柱手法治疗对慢性非特异性颈痛干预效果的Meta分析[J]. 《中国康复理论与实践》, 2022, 28(2): 150-164. |
| [9] | 柴良伟,刘华,黄秋玉,孙喜妹,李凯洋,马景. 治疗性运动对功能性踝关节不稳姿势控制和踝周肌肉功能影响的Meta分析[J]. 《中国康复理论与实践》, 2022, 28(11): 1278-1287. |
| [10] | 李欣欣,刘卉,马沐佳. 太极拳与其他运动降低老年人跌倒风险的Meta分析[J]. 《中国康复理论与实践》, 2022, 28(10): 1169-1177. |
| [11] | 柯竟悦,马圣楠,张晓慧,李古强. 青少年特发性脊柱侧凸患者静态站立及步行时生物力学变化的Meta分析[J]. 《中国康复理论与实践》, 2022, 28(10): 1178-1189. |
| [12] | 刘阳,张孝权,王恒,齐莉萍. 虚拟现实技术对帕金森病患者综合平衡能力改善的Meta分析[J]. 《中国康复理论与实践》, 2021, 27(9): 1048-1058. |
| [13] | 蔡倩,张溪,荆纯祥,蔡书宾,郭明凯,李际强. 弹性抗阻运动对慢性阻塞性肺疾病康复疗效的Meta分析[J]. 《中国康复理论与实践》, 2021, 27(8): 913-922. |
| [14] | 李玲玲,于莹,贾雨琦,黄海量. 脑机接口对脑卒中后上肢运动功能效果的Meta分析[J]. 《中国康复理论与实践》, 2021, 27(7): 765-773. |
| [15] | 郭辉,王剑桥,苏国栋,王华伟,樊华,樊祥德,张诗麟,刘洋,王月,吕雪琴,刘惠林. 神经肌肉本体感觉促进疗法对脑卒中患者平衡、运动和日常生活活动效果的Meta分析[J]. 《中国康复理论与实践》, 2021, 27(5): 530-541. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
|
||