


Chinese Journal of Rehabilitation Theory and Practice ›› 2025, Vol. 31 ›› Issue (5): 553-560.doi: 10.3969/j.issn.1006-9771.2025.05.008
Previous Articles Next Articles
WANG Mei1( ), ZHU Wenping2
), ZHU Wenping2
Received:2025-04-23
Published:2025-05-25
Online:2025-05-26
Contact:
WANG Mei, E-mail: wangmeipku@qq.com
Supported by:CLC Number:
WANG Mei, ZHU Wenping. Health benefits of physical activity in patients with type 2 diabetes: a systematic review of systematic reviews[J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(5): 553-560.
Table 1
PICO framework"
| 人群 | 干预 | 比较 | 结局 |
|---|---|---|---|
| 成人T2DM患者 | 干预类型 AE RT CT (AE+RT) HIIT 干预剂量 总剂量(总时间,MET·min/周) 频率与时间组合 运动强度 HIIT高强度期与恢复期强度 干预模式 监督式 非监督式 部分监督 无监督 | 非运动对照组(常规护理/健康教育/无干预) 不同干预方式比较 不同实施模式比较 不同干预强度比较 监督与非监督模式比较 | 身体健康 血糖控制:HbA1c、空腹胰岛素等 CRF:VO2max/peak 肌力 心血管风险因素:血脂谱、血压 体质量/BMI 并发症风险、死亡率 心理健康 自我效能感 抑郁 健康行为 久坐行为 |
Figure 1
Flowchart of literature screening"
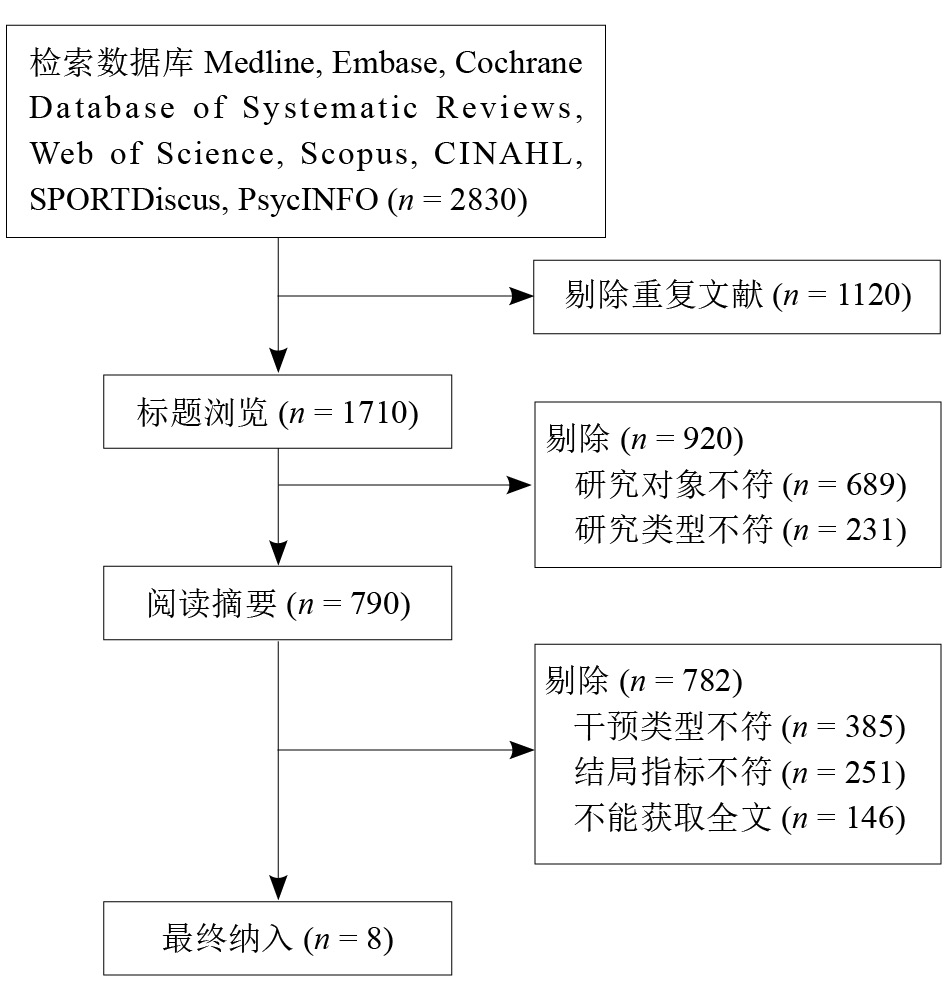
Table 2
Results of AMSTAR 2 of included literatures"
| 纳入文献 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 总体质量 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Maudet-Coulomb等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | - | √ | √ | √ | √ | √ | 高 |
| Gallardo-Gómez等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 高 |
| Grace等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 低 | |
| De Mello等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 低 | |
| Igarashi等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 高 |
| Jansson等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 高 |
| 王梅等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | - | √ | √ | √ | √ | √ | 高 |
| Pan等[ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 高 |
Table 3
Basic characteristics of included literatures"
| 纳入文献 | 国家 | 样本特征 | 干预类型 | 干预方案 | 比较 | 结局 |
|---|---|---|---|---|---|---|
| Maudet-Coulomb等[ | 法国 | 纳入研究:7项 样本量:n = 2096 平均年龄:62.6岁 健康状况:T2DM、高血压、血脂异常、冠心病或代谢综合征 | 身体活动:AE(如步行、游泳、有氧操等) 动机/自我效能干预:身体活动动机小组会议,心理学小组会议(促进个人对身体活动的信念和态度) 饮食干预:健康饮食和训练 | 频率:每次60~90 min,每周1~3次 强度:低~中等 时间:8~48周 模式:全程监督+部分监督 | 与非运动对照组比较 | 身体健康 血糖控制改善 体质量下降 心理健康 行走、运动和障碍自我效能感提高 健康行为 久坐时间减少 健康饮食行为增加 |
| Gallardo-Gómez等[ | 西班牙 | 纳入研究:126项 样本量:n = 6718 年龄:39~73岁 健康状况:T2DM | 身体活动:步行、AE | 频率:每次20~60 min,每周2~6次 强度:低~中等 时间:6~34周 模式:有监督 | 不同身体活动剂量比较 | 身体健康 血糖控制改善 体质量下降 心理健康 未提及 健康行为 未提及 |
| Grace等[ | 澳大利亚 | 纳入研究:27项 样本量:n = 1372 年龄:> 18岁 健康状况:T2DM | 身体活动:AE,如固定自行车、椭圆机等 | 频率:每次15~75 min,每周2~5次 强度:低~剧烈 时间:4~52周 模式:未提及 | 与非运动对照组比较 | 身体健康 HbA1c降低 血清胰岛素降低 体质量降低 CRF改善 心理健康 未提及 健康行为 未提及 |
| De Mello等[ | 巴西 | 纳入研究:20项 样本量:n = 738 年龄:43~69岁 健康状况:T2DM | 身体活动:HIIT (骑行、跑步、步行); MICT | 频率:每次20~60 min,每周2~6次 强度:中等~剧烈 时间:4~16周 模式:有监督 | 不同干预强度比较 | 身体健康 CRF提高 血糖控制改善 心血管疾病和糖尿病引起的并发症发生率和死亡率降低 心理健康 未提及 健康行为 未提及 |
| Igarashi等[ | 日本 | 纳入研究:48项 样本量:n = 2395 年龄:52~70岁 健康状况:T2DM | 身体活动:散步、慢跑或滑雪、气功、太极球、跑步机、椭圆机、划船机等 | 频率:每次20~60 min,每周2~5次 强度:低~剧烈 时间:12~39周 模式:未提及 | 不同干预方式比较 | 身体健康 血糖控制改善 心理健康 未提及 健康行为 久坐行为减少 |
| Jansson等[ | 澳大利亚 | 纳入研究:20项 样本量:n = 1489 年龄:55~85岁 健康状况:T2DM | 身体活动:RT,如卷腹、卧推、哑铃、滑轮、划船等 | 频率:每次10~30 min,每周4~12次 强度:低~剧烈 时间:8~48周 模式:有监督+部分监督 | 不同干预方式比较 | 身体健康 血糖控制改善 肌力改善 心理健康 未提及 健康行为 未提及 |
| 王梅等[ | 中国 | 纳入研究:10项 样本量: n = 24715 年龄:55~85岁 健康状况:T2DM | 身体活动:AE(跑步)、RT(卷腹、卧推、肩推、蹬腿等);CT 身体活动+饮食干预 | 频率:每次10~30 min,每周3~5次 强度:低~剧烈 时间:20~48周 模式:有监督+无监督 | 不同干预方式比较 | 身体健康 体质量、血压和多项生活质量指标改善 血糖控制改善 微血管并发症减少, 冠心病绝对风险降低 心理健康 抑郁改善 活力增加 健康行为 身体活动参与度提高 |
| Pan等[ | 中国 | 纳入研究:37项 样本量:n = 2208 年龄:55~72岁 健康状况:T2DM | 身体活动:AE、RT、CT | 频率:每次25~60 min,每周2~5次 强度:低~剧烈 时间:4~24周 模式:监督+无监督+部分监督 | 不同干预方式比较 不同身体活动模式比较 | 身体健康 HbA1c降低 体质量降低 收缩压降低 总胆固醇降低 心理健康 未提及 健康行为 未提及 |
| [1] | World Health Organization. Diabetes[EB/OL]. (2022-09-16) [2022-11-13]. https://www.who.int/zh/news-room/fact-sheets/detail/diabetes. |
| [2] | International Diabetes Federation. IDF diabetes atlas[M]. Brussels: International Diabetes Federation, 2021. |
| [3] | LI Y, TENG D, SHI X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study[J]. BMJ, 2020, 28(369): m997. |
| [4] | ELSAYED N A, ALEPPO G, ARODA V R, et al. Addendum. 2. Classification and diagnosis of diabetes: Standards of Care in Diabetes-2023. Diabetes Care 2023; 46(Suppl. 1): S19-S40[J]. Diabetes Care, 2023, 46(9): 1715. |
| [5] |
COLBERG S R, SIGAL R J, YARDLEY J E, et al. Physical activity/exercise and diabetes: a position statement of the American Diabetes Association[J]. Diabetes Care, 2016, 39(11): 2065-2079.
pmid: 27926890 |
| [6] |
RICHTER E, HARGREAVES M. Exercise, GLUT4, and skeletal muscle glucose uptake[J]. Physiol Rev, 2013, 93(3): 993-1017.
doi: 10.1152/physrev.00038.2012 pmid: 23899560 |
| [7] | WAKE A D. Antidiabetic effects of physical activity: how it helps to control type 2 diabetes[J]. Diabetes Metab Syndr Obes, 2020, 19(13): 2909-2923. |
| [8] |
VISSEREN F L J, MACH F, SMULDERS Y M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice[J]. Eur Heart J, 2021, 42(34): 3227-3337.
doi: 10.1093/eurheartj/ehab484 pmid: 34458905 |
| [9] | BULL F C, AL-ANSARI S S, BIDDLE S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour[J]. Br J Sports Med, 2020, 54(24): 1451-1462. |
| [10] | PAGE M J, MCKENZIE J E, BOSSUYT P M, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews[J]. BMJ, 2021, 29(372): n71. |
| [11] | SHEA B J, REEVES B C, WELLS G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both[J]. BMJ, 2017, 21(358): j4008. |
| [12] | MAUDET-COULOMB É, MARTIN-KRUMM C, TARQUINIO C, et al. Adapted physical activity interventions and motivational levers: what benefits for type 2 diabetics? A systematic review[J]. Health Sci Rep, 2024, 7(3): e1644. |
| [13] | GALLARDO-GÓMEZ D, SALAZAR-MARTÍNEZ E, ALFONSO-ROSA R M, et al. Optimal dose and type of physical activity to improve glycemic control in people diagnosed with type 2 diabetes: a systematic review and meta-analysis[J]. Diabetes Care, 2024, 47(2): 295-303. |
| [14] |
GRACE A, CHAN E, GIALLAURIA F, et al. Clinical outcomes and glycaemic responses to different aerobic exercise training intensities in type II diabetes: a systematic review and meta-analysis[J]. Cardiovasc Diabetol, 2017, 16(1): 37.
doi: 10.1186/s12933-017-0518-6 pmid: 28292300 |
| [15] | DE MELLO M B, RIGHI N C, SCHUCH F B, et al. Effect of high-intensity interval training protocols on VO(2)max and HbA1c level in people with type 2 diabetes: a systematic review and meta-analysis[J]. Ann Phys Rehabil Med, 2022, 65(5): 101586. |
| [16] | IGARASHI Y, AKAZAWA N, MAEDA S. The relationship between the level of exercise and hemoglobin A(1)c in patients with type 2 diabetes mellitus: a systematic review and meta-analysis[J]. Endocrine, 2021, 74(3): 546-558. |
| [17] | JANSSON A K, CHAN L X, LUBANS D R, et al. Effect of resistance training on HbA1c in adults with type 2 diabetes mellitus and the moderating effect of changes in muscular strength: a systematic review and meta-analysis[J]. BMJ Open Diabetes Res Care, 2022, 10(2): e002595. |
| [18] |
王梅, 廖婷, 陈建. 社区环境下2型糖尿病三种运动相关干预模式健康效益的系统综述[J]. 中国康复理论与实践, 2022, 28(11): 1288-1298.
doi: 10.3969/j.issn.1006-9771.2022.11.008 |
| WANG M, LIAO T, CHEN J. Health benefit of three exercise-related interventions for type 2 diabetes mellitus in community: a systematic review[J]. Chin J Rehabil Theory Pract, 2022, 28(11): 1288-1298. | |
| [19] |
PAN B, GE L, XUN Y Q, et al. Exercise training modalities in patients with type 2 diabetes mellitus: a systematic review and network meta-analysis[J]. Int J Behav Nutr Phys Act, 2018, 15(1): 72.
doi: 10.1186/s12966-018-0703-3 pmid: 30045740 |
| [20] | WRENCH E, RATTLEY K, LAMBERT J E, et al. There is no dose-response relationship between the amount of exercise and improvement in HbA1c in interventions over 12 weeks in patients with type 2 diabetes: a meta-analysis and meta-regression[J]. Acta Diabetol, 2022, 59(11): 1399-1415. |
| [21] | EDWARDS J, HOSSEINZADEH H. The impact of structured physical activity on glycaemic control in dia betes prevention programmes: a systematic review[J]. Proc Singapore Healthcare, 2017, 27(3): 193-204. |
| [22] | American College of Sports Medicine. ACSM's guidelines for exercise testing and prescription[M]. 11th ed. Philadelphia: Wolters Kluwer, 2021. |
| [23] | World Health Organization. WHO guidelines on physical activity and sedentary behaviour[M]. Geneva: World Health Organization, 2020. |
| [24] | World Health Organization. WHO package of essential noncommunicable (PEN) disease interventions for primary health care[M]. Geneva: World Health Organization, 2020. |
| [25] | WORMGOOR S G, DALLECK L C, ZINN C, et al. High-intensity interval training is equivalent to moderate-intensity continuous training for short- and medium-term outcomes of glucose control, cardiometabolic risk, and microvascular complication markers in men with type 2 diabetes[J]. Front Endocrinol (Lausanne), 2018, 28(9): 475. |
| [26] |
CASSIDY S, THOMA C, HOUGHTON D, et al. High-intensity interval training: a review of its impact on glucose control and cardiometabolic health[J]. Diabetologia, 2017, 60(1): 7-23.
pmid: 27681241 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
|
||