


Chinese Journal of Rehabilitation Theory and Practice ›› 2025, Vol. 31 ›› Issue (6): 666-673.doi: 10.3969/j.issn.1006-9771.2025.06.007
Previous Articles Next Articles
GU Yiqing1,2, CHENG Shupeng1,2, LI Yongqiang1,2, MAO Erli2, LI Jian'an1,2( )
)
Received:2025-02-26
Revised:2025-04-23
Published:2025-06-25
Online:2025-06-16
Contact:
E-mail: CLC Number:
GU Yiqing, CHENG Shupeng, LI Yongqiang, MAO Erli, LI Jian'an. Capping versus non-capping decannulation strategy in adult tracheostomized patients: a systematic review[J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(6): 666-673.
Table 1
PICO framework"
| 人群(Population) | 干预(Intervention) | 比较(Comparison) | 结局(Outcome) |
|---|---|---|---|
| 气管切开患者 | 干预场所 | 气管切开患者拔管的直接拔管策略和堵管策略的比较 堵管组(对照) 堵管≥ 24 h后实施拔管 | 拔管成功率 |
| 年龄≥ 18岁 | 医院(重症监护室、康复科病房) | 拔管时间 | |
| 康复服务中心 | 肺部感染 | ||
| 干预人员 | 不良反应 | ||
| 医生 | |||
| 护士 | |||
| 干预措施 | |||
| 对通过拔管评估的患者直接拔管,而不进行≥ 24 h的堵管 |

Figure 1
Flow diagram for literature screening"
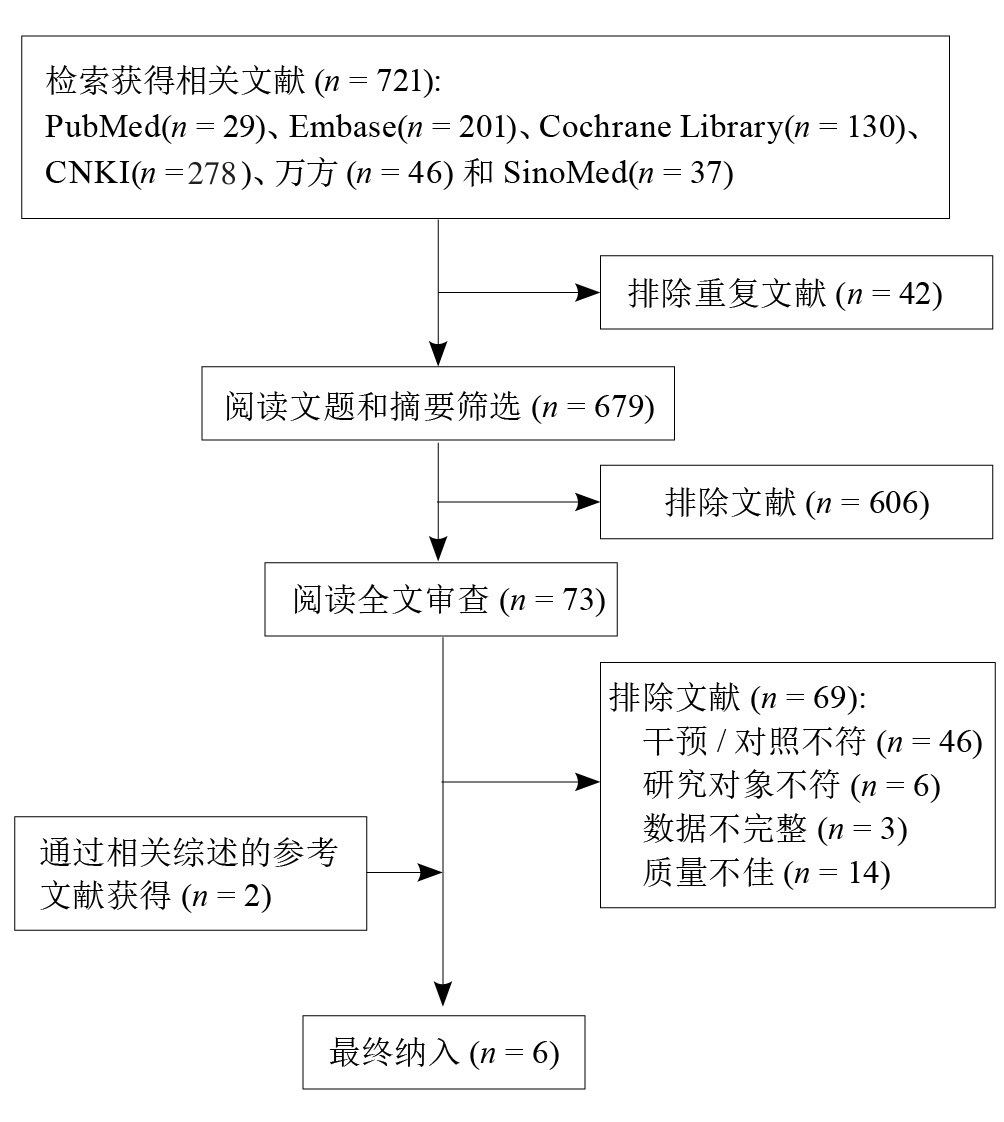
Table 2
Quality assessment of included studies"
| 纳入文献 | NOS评估 | Cochrane偏倚风险评估 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 研究人群选择 | 组间可比性 | 结果测量 | 总分 | 随机序列生成 | 分配隐藏 | 研究者与受试者盲法 | 结果评估盲法 | 数据 不完整 | 选择性报告 | 其他偏倚 | |
| Hernández Martínez等[ | + | + | ? | + | + | + | ? | ||||
| Shrestha等[ | ? | - | - | ? | ? | + | ? | ||||
| Cohen等[ | 3 | 1 | 2 | 6 | |||||||
| 廖圣芳等[ | 4 | 2 | 2 | 8 | |||||||
| 刘玲玲等[ | 3 | 2 | 2 | 7 | |||||||
| 夏嘉川等[ | 4 | 2 | 2 | 8 | |||||||
Table 3
Basical characteristics of included literatures"
| 纳入文献 | 研究类型 | 国家 | n | 女性比例/% | 年龄/岁 | 直接拔管组 | 堵管组 | 气管套管是否带气囊 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 措施 | n | 措施 | n | |||||||
| Hernández Martínez等[ | RCT | 西班牙 | 330 | 31.8 | 58.3±15.1 | 直接拔管 | 169 | 24 h堵管 | 161 | 是 |
| Shrestha等[ | RCT | 尼泊尔 | 118 | 16.9 | 34.0±13.2 | 直接拔管 | 50 | 24~48 h堵管 | 68 | NA |
| Cohen等[ | 病例对照研究 | 以色列 | 49 | 36.7 | 61.6±17.7 | 内镜检查后直接拔管 | 29 | 缩小管径后堵管 | 20 | 是 |
| 廖圣芳等[ | 病例对照研究 | 中国 | 122 | 27.9 | 38.0 | 直接拔管 | 61 | 24~48 h堵管 | 61 | 是 |
| 刘玲玲等[ | 病例对照研究 | 中国 | 52 | 26.9 | 45.3±15.5 | 直接拔管 | 26 | 24~48 h堵管 | 26 | 否 |
| 夏嘉川等[ | 病例对照研究 | 中国 | 74 | 29.7 | 63.2±11.5 | 直接拔管 | 37 | 部分堵管至全堵管 | 37 | NA |
Table 4
Decannulation assessments of included literatures"
| 纳入文献 | 拔管时意识状态 | 生命体征 | 咳嗽能力 | 吞咽能力 | 气道分泌物 | 气道通畅性 |
|---|---|---|---|---|---|---|
| Hernández Martínez等[ | 清醒 | + | + | 部分内镜检查 | 吸痰频率< 2次/8 h | 部分内镜检查 |
| Shrestha等[ | 部分有意识障碍 | + | + | - | + | 部分内镜检查 |
| Cohen等[ | - | + | + | 直接拔管组:内镜检查。堵管组:部分内镜检查 | ||
| 廖圣芳等[ | 部分有意识障碍 | + | + | - | 痰液明显减少> 2 d | - |
| 刘玲玲等[ | 部分有意识障碍 | + | + | - | + | - |
| 夏嘉川等[ | 部分有意识障碍 | + | + | + | - | 部分内镜检查 |
Table 5
GRADE quality of evidence for outcomes"
| 结局指标 | 纳入研究数/n | 研究的局限性 | 不一致性 | 间接性 | 不精确性 | 发表偏倚 | 证据质量 |
|---|---|---|---|---|---|---|---|
| 拔管成功率 | 6[ | 不严重 | 不严重 | 不严重 | 不严重 | 不严重 | 低级 |
| 拔管时间 | 3[ | 不严重 | 不严重 | 不严重 | 不严重 | 不严重 | 低级 |
| 肺部感染 | 3[ | 不严重 | 严重 | 不严重 | 严重 | 不严重 | 极低级 |
| 不良反应 | 3[ | 不严重 | 严重 | 不严重 | 不严重 | 不严重 | 极低级 |
| [1] | PANUGANTI B A, PANG J, FRANCIS D O, et al. Clinicodemographic predictors of tracheotomy tube size and decannulation: a multiinstitutional retrospective cohort study on tracheotomy[J]. Ann Surg, 2023, 277(5): e1138-e1142. |
| [2] | CHOTIRMALL S H, FLYNN M G, DONEGAN C F, et al. Extubation versus tracheostomy in withdrawal of treatment-ethical, clinical, and legal perspectives[J]. J Crit Care, 2010, 25(2): 360.e1-360.e8. |
| [3] | WALLACE S, MCGRATH B A. Laryngeal complications after tracheal intubation and tracheostomy[J]. BJA Educ, 2021, 21(7): 250-257. |
| [4] | SATALOFF R T. Clinical consensus statement: tracheostomy care[J]. Otolaryngol Head Neck Surg, 2013, 149(1): 174. |
| [5] | 中华医学会物理医学与康复学分会心肺康复学组, 中国康复医学会重症康复专业委员会. 成人气管切开拔管中国专家共识(下)[J]. 中华物理医学与康复杂志, 2023, 45(7): 577-584. |
| [6] |
中国残疾人康复协会神经康复专业委员会, 中国康复研究中心, 神经重症气管切开患者气道功能康复与管理专家共识(2024)[J]. 中国康复理论与实践, 2024, 30(8): 869-881.
doi: 10.3969/j.issn.1006-9771.2024.08.001 |
| Committee of Neurological Rehabilitation, China Association of Rehabilitation of Disabled Persons, China Rehabilitation Research Center. Expert consensus on rehabilitation and management of airway function for neurocritical patients with tracheotomy (2024)[J]. Chin J Rehabil Theory Pract, 2024, 30(8): 869-881. | |
| [7] | HERNÁNDEZ G, ORTIZ R, PEDROSA A, et al. La indicación de la traqueotomía condiciona las variables predictoras del tiempo hasta la decanulación en pacientes críticos[J]. Medicina Intensiva, 2012, 36(8): 531-539. |
| [8] | NOWAK A, MARTIN S, HÖHNE M, et al. Tracheal airway pressure in tracheostomy tube capping trials: an experimental study[J]. BMC Pulm Med, 2022, 22(1): 484. |
| [9] | PAGE M J, MCKENZIE J E, BOSSUYT P M, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews[J]. BMJ, 2021, 372: n71. |
| [10] | WELLS G A, TUGWELL P, O'CONNELL D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses[EB/OL]. [2025-02-26]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm. |
| [11] | 曾宪涛, 刘慧, 陈曦, 等. Meta分析系列之四:观察性研究的质量评价工具[J]. 中国循证心血管医学杂志, 2012, 4(4): 297-299. |
| [12] | HIGGINS J P, ALTMAN D G, GØTZSCHE P C, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials[J]. BMJ, 2011, 343: d5928. |
| [13] | 曾宪涛, 包翠萍, 曹世义, 等. Meta分析系列之三:随机对照试验的质量评价工具[J]. 中国循证心血管医学杂志, 2012, 4(3): 183-185. |
| [14] |
GUYATT G, OXMAN A D, AKL E A, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables[J]. J Clin Epidemiol, 2011, 64(4): 383-394.
doi: 10.1016/j.jclinepi.2010.04.026 pmid: 21195583 |
| [15] | HERNÁNDEZ MARTÍNEZ G, RODRIGUEZ M L, VAQUERO M C, et al. High-flow oxygen with capping or suctioning for tracheostomy decannulation[J]. N Engl J Med, 2020, 383(11): 1009-1017. |
| [16] |
SHRESTHA K K, MOHINDRA S, KUMAR SHRESTHA K. How to decannulate tracheostomised severe head trauma patients: a comparison of gradual vs abrupt technique.[J]. Nepal Med Coll J, 2012, 14(3): 207-211.
pmid: 24047017 |
| [17] | COHEN O, TZELNICK S, LAHAV Y, et al. Feasibility of a single-stage tracheostomy decannulation protocol with endoscopy in adult patients[J]. Laryngoscope, 2016, 126(9): 2057-2062. |
| [18] | 廖圣芳, 陈汉民, 张银清, 等. 重型颅脑损伤气管切开术后直接拔管的临床研究[J]. 中国综合临床, 2003, 19(12): 63-64. |
| [19] | 刘玲玲, 尤春景. 脑损伤患者气管切开术后直接拔管的临床研究[J]. 中国康复, 2014, 29(5): 359-361. |
| LIU L L, YOU C J. One-stage decannulation in brain damage patients with tracheotomy[J]. Chin J Rehabil, 2014, 29(5): 359-361. | |
| [20] |
夏嘉川, 罗忠纯, 郭祥奎, 等. 气管切开后拔管策略对拔管成功率的影响[J]. 中国康复理论与实践, 2018, 24(9): 1067-1071.
doi: 10.3969/j.issn.1006-9771.2018.09.016 |
| XIA J C, LUO Z C, GUO X K, et al. Comparison of ways of extubation after tracheotomy[J]. Chin J Rehabil Theory Pract, 2018, 24(9): 1067-1071. | |
| [21] | PANDIAN V, MILLER C R, SCHIAVI A J, et al. Utilization of a standardized tracheostomy capping and decannulation protocol to improve patient safety[J]. Laryngoscope, 2014, 124(8): 1794-1800. |
| [22] | CERIANA P, CARLUCCI A, NAVALESI P, et al. Weaning from tracheotomy in long-term mechanically ventilated patients: feasibility of a decisional flowchart and clinical outcome[J]. Intensive Care Med, 2003, 29(5): 845-848. |
| [23] | STELFOX H T, CRIMI C, BERRA L, et al. Determinants of tracheostomy decannulation: an international survey[J]. Crit Care, 2008, 12(1): R26. |
| [24] |
MUSSA C C, GOMAA D, ROWLEY D D, et al. AARC clinical practice guideline: management of adult patients with tracheostomy in the acute care setting[J]. Respir Care, 2021, 66(1): 156-169.
doi: 10.4187/respcare.08206 pmid: 32962998 |
| [25] | Korean Bronchoesophagological Society Guideline Task Force, NAM I C, SHIN Y S, et al. Guidelines for tracheostomy from the Korean bronchoesophagological society[J]. Clin Exp Otorhinolaryngol, 2020, 13(4): 361-375. |
| [26] | TROUILLET J L, COLLANGE O, BELAFIA F, et al. Tracheotomy in the intensive care unit: guidelines from a French expert panel[J]. Ann Intensive Care, 2018, 8(1): 37. |
| [27] | EPSTEIN S K. Anatomy and physiology of tracheostomy[J]. Respir Care, 2005, 50(4): 476-482. |
| [28] | 胡银, 青晨, 袁梅, 等. 神经外科气管切开患者拔管指征的最佳证据总结[J]. 中华现代护理杂志, 2023, 29(21): 2847-2854. |
| HU Y, QING C, YUAN M, et al. Best evidence summary of indications for extubation in neurosurgical tracheotomy patients[J]. Chin J Mod Nurs, 2023, 29(21): 2847-2854. | |
| [29] | 牛光宇, 连素娜, 刘仲楠, 等. 全国各级医疗机构关于气管切开套管拔管临床实践情况的调查[J]. 中华结核和呼吸杂志, 2022, 45(8): 762-767. |
| NIU G Y, LIAN S N, LIU Z N, et al. A survey on clinical practice of tracheostomy decannulation in medical institutions at all levels across the country[J]. Chin J Tuberc Respir Dis, 2022, 45(8): 762-767. | |
| [30] | 丁玉菊, 徐绍侠, 张伟, 等. 神经重症气管切开患者拔管临床指征的Meta分析[J]. 中华危重病急救医学, 2019, 31(11): 1378-1383. |
| DING Y J, XU S X, ZHANG W, et al. Indication of tracheostomy extubation in patients with severe neuropathy: a meta-analysis[J]. Chin Crit Care Med, 2019, 31(11): 1378-1383. | |
| [31] | 徐锐, 张济源, 覃家德, 等. 气管切开术后245例直接拔管的认识和体会[J]. 中国临床神经外科杂志, 2012, 17(4): 244-245. |
| [32] |
DAWSON D. Essential principles: tracheostomy care in the adult patient[J]. Nurs Crit Care, 2014, 19(2): 63-72.
doi: 10.1111/nicc.12076 pmid: 24529106 |
| [33] | NINAN A, GRUBB L M, BRENNER M J, et al. Effectiveness of interprofessional tracheostomy teams: a systematic review[J]. J Clin Nurs, 2023, 32(19/20): 6967-6986. |
| [34] | KUTSUKUTSA J, KUUPIEL D, MONORI-KISS A, et al. Tracheostomy decannulation methods and procedures for assessing readiness for decannulation in adults: a systematic scoping review[J]. Int J Evid Based Healthc, 2019, 17(2): 74-91. |
| [35] |
SANTUS P, GRAMEGNA A, RADOVANOVIC D, et al. A systematic review on tracheostomy decannulation: a proposal of a quantitative semiquantitative clinical score[J]. BMC Pulm Med, 2014, 14: 201.
doi: 10.1186/1471-2466-14-201 pmid: 25510483 |
| [36] | SANCHEZ-GUERRERO J A, GUERLAIN J, CEBRIÀ I IRANZO M À, et al. Expiratory airflow obstruction due to tracheostomy tube: a spirometric study in 50 patients[J]. Clin Otolaryngol, 2020, 45(5): 703-709. |
| [37] |
CARTER A, FLETCHER S J, TUFFIN R. The effect of inner tube placement on resistance and work of breathing through tracheostomy tubes: a bench test[J]. Anaesthesia, 2013, 68(3): 276-282.
doi: 10.1111/anae.12094 pmid: 23278349 |
| [38] |
WARNECKE T, SUNTRUP S, TEISMANN I K, et al. Standardized endoscopic swallowing evaluation for tracheostomy decannulation in critically ill neurologic patients[J]. Crit Care Med, 2013, 41(7): 1728-1732.
doi: 10.1097/CCM.0b013e31828a4626 pmid: 23774336 |
| [39] |
MORRIS L L. Capping a cuffed tracheostomy tube[J]. Crit Care Nurse, 2012, 32(2): 12-13.
doi: 10.4037/ccn2012391 |
| [40] |
VILLALBA D, FELD V, LEIVA V, et al. Effect of tracheostomy tube on work of breathing: comparison of pre- and post-decannulation[J]. Int J Crit Illn Inj Sci, 2016, 6(3): 98-102.
pmid: 27722109 |
| [41] | SHI Z H, JONKMAN A, DE VRIES H, et al. Expiratory muscle dysfunction in critically ill patients: towards improved understanding[J]. Intensive Care Med, 2019, 45(8): 1061-1071. |
| [42] | ZANATA IDE L, SANTOS R S, HIRATA G C. Tracheal decannulation protocol in patients affected by traumatic brain injury[J]. Int Arch Otorhinolaryngol, 2014, 18(2): 108-114. |
| [43] |
GALLICE T, CUGY E, BRANCHARD O, et al. Predictive factors for successful decannulation in patients with tracheostomies and brain injuries: a systematic review[J]. Dysphagia, 2024, 39(4): 552-572.
doi: 10.1007/s00455-023-10646-2 pmid: 38189928 |
| [44] |
DZIEWAS R, STELLATO R, VAN DER TWEEL I, et al. Pharyngeal electrical stimulation for early decannulation in tracheotomised patients with neurogenic dysphagia after stroke (PHAST-TRAC): a prospective, single-blinded, randomised trial[J]. Lancet Neurol, 2018, 17(10): 849-859.
doi: S1474-4422(18)30255-2 pmid: 30170898 |
| [45] | LANINI B, BINAZZI B, ROMAGNOLI I, et al. Tracheostomy decannulation in severe acquired brain injury patients: the role of flexible bronchoscopy[J]. Pulmonology, 2023, 29(Suppl 4): S80-S85. |
| [46] | MARTIN K A, COLE T D K, PERCHA C M, et al. Standard versus accelerated speaking valve placement after percutaneous tracheostomy: a randomized controlled feasibility study[J]. Ann Am Thorac Soc, 2021, 18(10): 1693-1701. |
| [1] | WANG Mei, ZHU Wenping. Health benefits of physical activity in patients with type 2 diabetes: a systematic review of systematic reviews [J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(5): 553-560. |
| [2] | YE Lü, CHANG Jing, LING Hairun. Effect of exercise intervention on internet behavioral addictions: a systematic review of systematic reviews [J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(4): 431-440. |
| [3] | ZHU Zhiqiang, XU Qiaoling, SHAO Xueyun. Health benefits of physical activity for obese and overweight children: a systematic review of systematic reviews [J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(3): 296-305. |
| [4] | CAI Qian, ZHANG Xi, SU Hairong, LIU Na, HUANG Ying, LI Jiqiang, XIA Jin'gen, ZHENG Decai. Inspiratory muscle training for weaning outcomes in patients with weaning failure: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(3): 306-313. |
| [5] | XU Xiaohong, ZHONG Xiaoke, SUN Siyi, ZHANG Qi, CHENG Huaichun. Psychological benefits of art therapy for older adults with mild cognitive impairment: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2025, 31(2): 165-171. |
| [6] | YANG Wenrui, CUI Sidong, ZENG Li. Effect of virtual and augmented reality on cognition, emotion and adaptive behavior in children and adolescents with autism spectrum disorder: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(9): 1026-1033. |
| [7] | ZHOU Jing, ZHANG Xiaoxiao, DING Zhongbing, CHEN Jianchao, WEI Xingxing, LIN Shuqi. Effect of speech and language rehabilitation on children with intellectual and developmental disabilities: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(8): 894-902. |
| [8] | YANG Jiakun, ZHANG Xiaoxia. Effect of adapted physical activity on functioning, activity and participation in children with intellectual and developmental disabilities: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(7): 768-777. |
| [9] | TANG Letian, HUANG Zhaoxin, LIU Chao, XIAO Xiaofei. Effect of high blood flow restriction training on patients after anterior cruciate ligament reconstruction: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(7): 789-796. |
| [10] | WEI Xiaowei. Effect of digital empowerment techniques on physical activity and health for children with intellectual and developmental disabilities: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(5): 497-504. |
| [11] | WANG Hongzhi, YANG Jian. Application of virtual reality technology in physical activity and health of children and adolescents with cerebral palsy: a systematic review of systematic reviews [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(5): 505-512. |
| [12] | ZHONG Xiaoke, WANG Qi, CHANG Siqin, JIANG Changhao. Effect of long-term physical activity on executive function of children with autism spectrum disorder: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(5): 535-542. |
| [13] | WU Jiaming, ZHANG Qing, WU Aihong. Functioning, health and developmental benefits of music interventions for children and adolescents with intellectual and developmental disabilities: a systematic review of systematic reviews [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(5): 543-553. |
| [14] | XI Yue, YANG Jian. Physical activity intervention and its health benefits for children and adolescents with cerebral palsy: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(2): 157-167. |
| [15] | ZHANG Haoyuan, TIAN Gang, LI Xuefeng, LI Hongjiang, MIN Hongwei, TANG Peng, ZHANG Rui, GU Rui, LIU Kemin. Influence of clinical and rehabilitation characteristics on prognosis of diabetic foot amputees: a systematic review [J]. Chinese Journal of Rehabilitation Theory and Practice, 2024, 30(11): 1281-1290. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
|
||